Gateways: International Journal of Community Research and Engagement
Vol. 19, No. 1
March 2026
PRACTICE-BASED ARTICLE
Implementation of the North Carolina American Indian Adult Tobacco Survey: A Community-Government-University Collaboration
Rachel Denlinger-Apte1,2,3, Tomi Akinyemiju3,4,5, Peggy Ammons6, Ronny Bell3,7,8,9,10, Laury Chavis6,7, Ryan Dial3,7,9,11, Courtney Graham6, Emily Harwood1,3, Courtney Heck12, Sally Herndon12, Kayla Hicks1, Charlene Hunt1,3,7, Darcy Lockhart1, Jim Martin12, Lu McCraw12,13, Yadu Raveendran3,4, Greg Richardson6,14, Ana Salas3,9,11 and Stephanie Wheeler3,9,10,15
1 Wake Forest University School of Medicine
2 Atrium Health Wake Forest Baptist Comprehensive Cancer Center
3 Southeastern American Indian Cancer Health Equity Partnership (SAICEP)
4 Duke Cancer Institute
5 Duke University School of Medicine
6 NC Commission of Indian Affairs, NC Department of Administration
7 Lumbee Tribe
8 Eshelman School of Pharmacy
9 Lineberger Comprehensive Cancer Center
10 University of North Carolina – Chapel Hill
11 UNC School of Medicine
12 Division of Public Health, NC Department of Health and Human Services
13 Otoe-Missouria Tribe of Indians, Red Rock, Oklahoma
14 Haliwa-Saponi Indian Tribe
15 Gillings School of Public Health
Corresponding author: Rachel Denlinger-Apte, rachel.denlinger@wfusm.edu
DOI: https://doi.org/10.5130/fx4kp415
Article History: Received 06/06/2025; Revised 01/11/2025; Accepted 17/11/2025; Published 03/2026
Abstract
Commercial tobacco use remains a leading contributor to the cancer burden in the United States and disproportionately affects historically marginalised communities including American Indians. National surveys estimate current cigarette smoking prevalence for American Indian adults is 27 per cent; however, state-level and tribe-specific data are limited. North Carolina is home to seven state-recognised tribes, one federally-recognised tribe and four Urban Indian Organisations with approximately 300 000 residents identifying as American Indian. We conducted a commercial tobacco use survey with and for tribal leaders and communities in North Carolina to assess overall tobacco use among American Indian residents and by tribal affiliation. Next steps include prioritising the dissemination of our results to tribal leaders, community members, state regulators and academic partners. This will guide the development of policy, systems and environmental changes to reduce commercial tobacco use among American Indians. Here, we highlight our community-academic-government collaboration supporting implementation of the North Carolina American Indian Adult Tobacco Survey. Our research team includes members from multiple tribes, universities and state organisations across North Carolina.
Keywords
Indigenous Health; American Indian Populations; Commercial Tobacco Use; Online Surveys; Community-Engagement; Academia; Government
Introduction
Despite significant progress over the last 50 years, commercial tobacco use remains a leading cause of disease and premature death in the United States (US) that disproportionately affects marginalised populations (US Department of Health and Human Services 2014). Data from the 2020 National Health Interview Survey estimated over 27 per cent of American Indian/Alaska Native adults smoke cigarettes, which is the highest smoking rate among racial and ethnic groups (Cornelius et al. 2022). Further, American Indian/Alaska Native adults have had the highest smoking prevalence since 1978 (US Food and Drug Administration 2023). This sustained inequity results from decades of tobacco industry marketing and manipulation, historical political injustices banning use of traditional tobacco and contemporary experiences of stress, trauma and discrimination (D’Silva, O’Gara & Villaluz 2018; Lempert & Glantz 2019). Therefore, reducing commercial tobacco use in this population is critical for achieving equity through improving health, wellbeing and social justice.
However, one challenge of conducting research about tobacco control and cessation among tribal communities is the limited data available from this priority population. Even when included in nationally-representative surveys, the number of respondents identifying as American Indian/Alaska Native persons is usually quite low relative to other racial categories and typically does not include information about tribal affiliation. For example, in the 2022 Behavioral Risk Factor Surveillance System survey administered in North Carolina, the number of American Indian/Alaska Native respondents was quite low (n=82), which potentially led to unreliable estimates, and no information about tribal affiliation of the respondents was reported. Indeed, 14.5 per cent of the overall sample reported current cigarette smoking but smoking prevalence estimates for American Indian/Alaska Native respondents were not included, likely due to the small sample size. Thus, typical survey data treat American Indian/Alaska Native persons as one homogeneous population instead of the diverse group of tribal communities that exist across the country and often cannot provide critical data due to the small number of American Indian/Alaska Native respondents. Without accurate and tribe-specific data, those who are responsible for the allocation of resources may not be able to provide the support required to address the enduring and significant commercial tobacco-related health disparities that exists for American Indian/Alaska Native persons. Additionally, there is variation in commercial tobacco use among American Indians/Alaska Natives across the different geographic regions in the US, so national prevalence estimates may not accurately reflect local populations (Daley et al. 2010).
Culturally, tobacco holds a significant and sacred place in Native American/Indigenous culture (McCraw 2023). Across Turtle Island (North America), Native Americans use sacred or traditional tobacco, revering it highly as medicine and using it during prayer. To receive sacred or traditional tobacco is an honour and shows great respect for the person receiving it. Before colonisation, sacred tobacco was used for ceremonial and cultural practices to promote wellness for Indigenous people and communities (Henderson et al. 2022). Importantly, sacred or traditional tobacco use is not associated with increased risk of addiction or negative health consequences, as it is typically not inhaled or used recreationally. Additionally, the process of cultivating sacred or traditional tobacco does not include use of pesticides, additives or other harmful chemicals found in commercial tobacco production. Therefore, any efforts to reduce commercial tobacco use among American Indians must acknowledge the importance of sacred or traditional tobacco usage.
North Carolina is home to seven state-recognised tribes, one federally-recognised tribe and four Urban Indian Organisations (see Figure 1). According to the 2020 US Census data, approximately 300 000 North Carolina residents identify as American Indian, which is the largest tribal population east of the Mississippi River. North Carolina is also heavily reliant on its agricultural industry, especially in rural areas where many of the state’s tribal homelands are located. North Carolina leads the nation in tobacco production, producing more than double the rate of the second leading state, Kentucky (Shahbandeh 2024). Further, in 2024, North Carolina received four ‘F’ and one ‘D’ grades from the American Lung Association for its efforts to implement tobacco prevention and cessation policies (American Lung Association 2024).
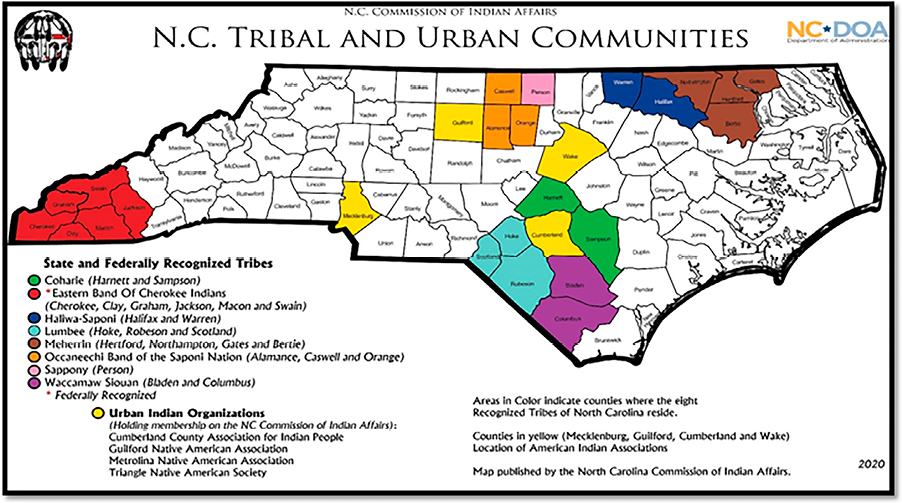
Figure 1. Map of North Carolina’s tribal and urban communities
Given prior survey limitations, our primary objective is to conduct a commercial tobacco use prevalence survey with and for tribal communities in North and South Carolina to assess current use among American Indian residents and by tribal affiliation. Our research team includes members from multiple tribes, universities and state organisations across North Carolina. We enrolled survey respondents who were at least 18 years of age or older, identified as American Indian and lived in North or South Carolina. The survey was expanded to include tribal residents in South Carolina because the Wake Forest University School of Medicine (Wake Forest) cancer catchment area (of which Dr Rachel Denlinger-Apte is a member) now includes the Catawba Nation in south-western South Carolina. Once data analysis has concluded, our findings will be shared with tribal leaders and state regulators to identify areas of need for each tribe with respect to supporting commercial tobacco prevention and cessation efforts. Additionally, we will develop health communication materials (for example, infographics and social media posts) to disseminate our findings widely across tribal communities. Here, we describe our collaborative journey, shared successes and lessons learned with respect to implementing a survey among tribal communities.
Establishing and leveraging multiple collaborations
Although some collaborations pre-date the current project, the initial step of this commercial tobacco control survey occurred in 2019 with a community-engagement project conducted by the Maya Angelou Research Center for Healthy Communities at Wake Forest and the North Carolina American Indian Health Board, called ‘Native Pathways to Health’ (Irby et al. 2021). This project conducted talking circles, a traditional method for problem-solving in tribal communities, to identify health needs for American Indian adults living in North Carolina. Ms Charlene Hunt, a member of the Lumbee Tribe, facilitated the talking circles. Overall, members of the talking circles identified cancer as a major concern for their tribes. Commercial tobacco use and/or tobacco-related health concerns such as cardiovascular disease also emerged during the talking circles.
In 2021, Dr Denlinger-Apte, a tobacco control researcher, received a Career Development Award from the Wake Forest Cancer Center to conduct focus groups among tribal communities in North Carolina to discuss proposed federal regulations for commercial tobacco products. Dr Ronny Bell, a member of the Lumbee Tribe, provided academic mentorship on the project while Ms Hunt provided expertise on tribal engagement based on her prior work on the Native Pathways to Health project. Ms Emily Harwood joined Wake Forest as the project manager for this qualitative research study. Prior to her employment at Wake Forest, she worked in a local health department in North Carolina and upon starting the qualitative research study, Ms Harwood reached out to her former colleagues who were also working on American Indian-related initiatives. From this connection, a monthly American Indian Commercial Tobacco Use Working Group was established between researchers at Wake Forest (Dr Denlinger-Apte, Ms Harwood and Ms Hunt) and employees at the North Carolina Tobacco Prevention and Control Branch (Ms Sally Herndon, Ms Courtney Heck, Ms Lu McCraw and Mr Jim Martin). The working group initially shared areas of interest and current research/policy projects related to commercial tobacco use among American Indian residents but eventually identified the dire need for tribe-specific commercial tobacco use data, which aligned with the communities’ concerns discussed during the Native Pathways to Health project. Also in 2021, researchers from the three National Cancer Institute-designated Comprehensive Cancer Centers in North Carolina – Wake Forest, Duke Cancer Institute (Duke) and the University of North Carolina Lineberger Comprehensive Cancer Center (UNC) – established a new collaboration focused on understanding and eliminating cancer-related health disparities among tribal communities in North Carolina, called the ‘Southeastern American Indian Cancer Health Equity Partnership’ (SAICEP) (Bell et al. 2025). At the time, Dr Tomi Akinyemiju (Duke), Dr Bell (Wake Forest) and Dr Stephanie Wheeler (UNC) each led the Community Outreach and Engagement core for their respective cancer centers and became the founding co-leaders of SAICEP. Leveraging findings from the Native Pathways to Health project, the SAICEP team obtained a collaborative research grant from the V Foundation (D2022-012; PI: Stephanie Wheeler) focused on understanding cancer-related health disparities among American Indian residents in North Carolina. When Dr Bell moved his faculty employment from Wake Forest to UNC in early 2022, Dr Denlinger-Apte temporarily filled in as Wake Forest’s leadership role for SAICEP.
As a result of this collective work and the clear gap in state-level data for commercial tobacco use among American Indians, the North Carolina American Indian Adult Tobacco Survey was born. The team then began the process of establishing a potential funding source to support the project.
Survey funding
To implement the survey, we needed to identify a funding source since our initial commercial tobacco working group relied on volunteers’ efforts. In 2022, Dr Denlinger-Apte and Dr Bell submitted a grant application but the grant application was not selected for funding after the peer-review process. Ms Herndon, Head of the Tobacco Prevention and Control Branch, North Carolina Division of Public Health and Principal Investigator for the Centers for Disease Control and Prevention’s COVID-19 Health Disparities grant (6 NH75OT000028-01-02) to the North Carolina Department of Health and Human Services identified these funds as an appropriate funding source, as people who smoke are more likely to suffer severe illness with COVID-19, including emergency department visits, hospitalisation and death (North Carolina Department of Health and Human Services 2021). She presented the research plan to the Centers for Disease Control and Prevention’s grants management team and received approval to use the funds for the planned survey. Following this, the North Carolina Tobacco Prevention and Control Branch contracted with the North Carolina Commission of Indian Affairs, part of the North Carolina Department of Administration, to administer the survey (more details below). Additionally, in 2023, the SAICEP team applied for and received funding from the V Foundation (D2023-005; PI: Tomi Akinyemiju) that included money to support survey implementation, primarily to purchase additional gift cards for respondents. With funding secured, the unique North Carolina American Indian Adult Tobacco Survey project team was fully formed (see Figure 2).
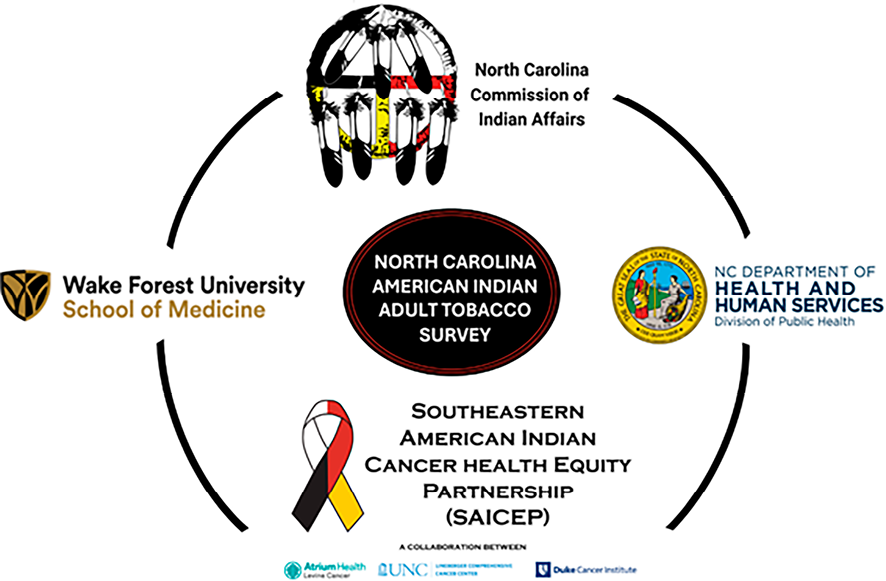
Figure 2. North Carolina American Indian Adult Tobacco Survey project team
Survey development and implementation
For survey development, the Centers for Disease Control and Prevention’s American Indian Adult Tobacco Survey – 2018 Version was adapted to create the North Carolina American Indian Adult Tobacco Survey. Because our survey recruitment relied primarily on speaking with tribal members during community events, we aimed for the survey completion time to be between 10–15 minutes, which required a reduction in the number of survey items administered. The survey assessed lifetime and current use of several commercial tobacco products (for example, cigarettes, e-cigarettes, cigars, chewing tobacco and so forth) and related constructs (for example, age at first use, e-liquid flavour preference) as well as questions about use of sacred or traditional tobacco. To incorporate SAICEP’s mission into the survey, we also added questions about awareness and uptake of cancer screenings. Finally, we included a few questions about potential commercial tobacco regulations given the initial interests of the Commercial Tobacco Working Group. Members from all collaborating organisations (North Carolina Commission of Indian Affairs, North Carolina Tobacco Prevention and Control Branch, SAICEP and Wake Forest) had the opportunity to review the survey and provide feedback on which constructs to maintain and which to exclude as well as ensure use of culturally appropriate language for the population. Thus, our final survey included 86 questions (see Table 1), although only a single respondent who reported current use of all commercial tobacco products would answer all 86 questions.
The survey implementation team prioritised its organisational infrastructure from the onset to ensure tribal leadership and representation throughout and collection of sufficient data to understand the impact of commercial tobacco use among American Indians in North and South Carolina comprehensively (see Figure 3). To accomplish this, the team from the North Carolina Commission of Indian Affairs spearheaded the leadership of the survey and led all efforts in disseminating the survey. The North Carolina Commission of Indian Affairs served as the face of the survey both externally in the community and internally within our team to ensure the survey remained a product created by tribal members for tribal members. Ms Laury Chavis hired tribal members from across the state to work as survey specialists. Survey specialists were trusted members in their respective communities and worked to elevate the voices of their fellow tribal members through the completion of the survey. Survey specialists represented four of the eight tribes in North Carolina and covered all tribal geographic regions in the state. Ms Chavis, the survey director, a member of the Lumbee tribe, provided survey implementation oversight as well as supervision to the survey specialists (Initially, Ms Peggy Ammons and Ms Courtney Graham). Ms Harwood provided protocol training for survey implementation prior to launching the survey as well as access to Collaborative Institutional Training Initiative Program responsible conduct of research training modules (www.citiprogram.org) for ensuring ethical research practice. All tribal staff received certificates in basic human subject research training to be better educated on research ethics. The North Carolina Commission of Indian Affairs and Wake Forest teams held weekly check-in meetings to discuss survey progress, upcoming community recruitment events and any successes and challenges experienced by the survey specialists during the previous week. Ms Kayla Hicks, a Wake Forest associate project manager, organised this weekly meeting, which provided the opportunity to discuss community reactions to the survey as well as any other concerns related to implementation to ensure tribal voices remained at the forefront of this project.
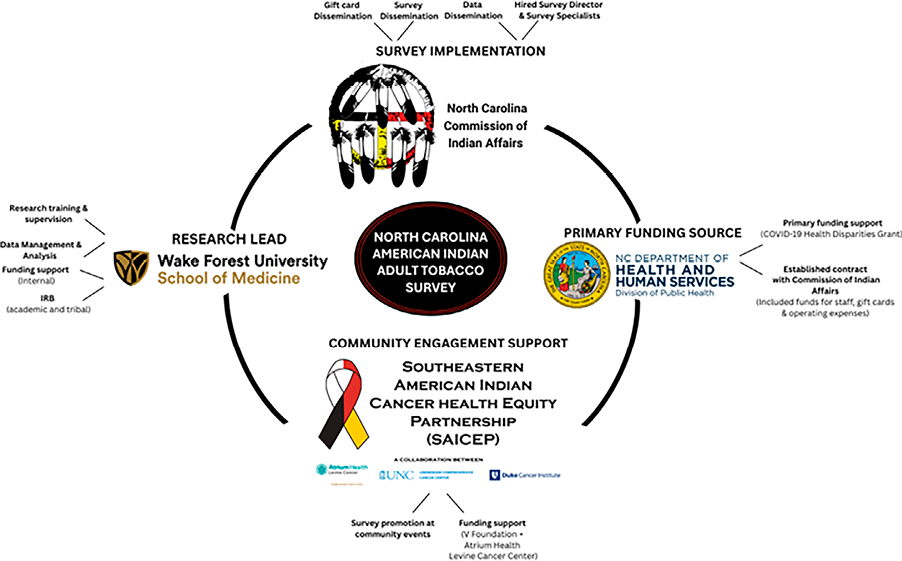
Figure 3. Organisational structure of the survey team and corresponding roles of each partner
The survey specialists attended a variety of community events such as tribal Pow Wows, homecomings, health fairs and culture classes to connect with fellow tribal members, explain the purpose of the survey and answer any questions individuals had. For those interested in completing the survey, the survey specialists provided access to the survey in REDCap, an online data collection platform, via flyers with Quick Response codes. Respondents could complete the survey during the event, with the support of the survey specialists if needed, or at a more convenient time later. Respondents could elect to receive a $25 gift card for completing the survey by providing their contact information after completion of the survey. The North Carolina Commission of Indian Affairs obtained the gift cards from a Native-owned community bank and mailed gift cards to respondents approximately once per month. The survey officially launched in June 2023 during the annual Lumbee Tribal Homecoming event. The survey specialists attended over 80 community events (see Table 2), resulting in 2771 survey completers with representation from all eight North Carolina tribes and more than 50 other North American tribes.
Wake Forest maintained survey management and oversight including organising weekly team meetings, obtaining Institutional Review Board approvals for the survey (Wake Forest: IRB00094932; Eastern Band of Cherokee Indian: MIRB#118), developing and testing the survey in REDCap (online data collection software), creating survey flyers and social media advertisements, safely sharing respondent contact information to the North Carolina Commission of Indian Affairs staff for gift card mailings, cleaning and analysing the survey data and presenting recruitment updates during team meetings. Additionally, survey respondents from South Carolina received their survey incentives directly from Wake Forest, rather than the North Carolina Commission of Indian Affairs, since funding to include tribal members in South Carolina came directly from Wake Forest.
Data sovereignty and dissemination of results
Our primary goal now that the survey is complete is to provide tribe-specific results to each tribe, where appropriate (for example, sample size by tribe is sufficiently large to ensure confidentiality). Tribe-specific data will only be shared outside the survey team once approval has been granted from each respective tribe. A Data Use Agreement is in place between the North Carolina Commission of Indian Affairs and Wake Forest to allow for data protection and shared ownership. The survey data may be shared by members of the survey team at conferences and presentations once approved by Wake Forest and the North Carolina Commission of Indian Affairs to ensure data is portrayed accurately and respectfully. We intend to schedule community presentations for each tribe to present their specific results in the coming year and will obtain permission to share the tribe’s findings at that time. Once approval has been granted, we will create culturally-relevant infographics highlighting data across each tribe to share at all community events attended by the North Carolina Commission of Indian Affairs. We will also develop a social media campaign to disseminate our findings widely. The social media campaign will only share collective findings across all tribes and will not share tribe-specific data to ensure data sovereignty and accord respect to each tribe.
To date, we have presented workshops focused more generally on cancer and commercial tobacco use in tribal communities during the annual North Carolina American Indian Unity Conferences (March 2023, March 2024) and the annual North Carolina Native American Youth Organisation Conferences (June 2023, June 2024). Next, we will use the data to determine the areas of need with regard to tobacco prevention and cessation. Together, we will identify additional resources and opportunities to support tribal communities as well as develop novel, culturally-relevant interventions to reduce the burden of commercial tobacco use among American Indians in North and South Carolina.
Lessons learned
The understandable distrust of academia participants experience given the historical research injustices and traumas experienced by them is challenging to overcome. The success of this survey is the result of the productive collaboration between all groups. The unique infrastructure and emphasis on American Indian leadership of the survey has allowed tribal voices to remain at the forefront of the project resulting in trust and participation in the survey. Funding support and leadership provided by the North Carolina Tobacco Prevention and Control Branch combined with the academic and regulatory support provided by Wake Forest and SAICEP established an essential and strong foundation for the project, allowing the North Carolina Commission of Indian Affairs to focus on elevating tribal voices through survey responses. Below we describe several important lessons learned with respect to the successful administration of the survey.
One major challenge was administering a tobacco survey in a state growing the most commercial tobacco (Shahbandeh 2024) and with the second-largest commercial tobacco company in the US (https://www.reynoldsamerican.com/building-brands/). Anecdotally, many survey respondents informed our survey specialists about the economic impact of commercial tobacco agriculture or manufacturing within their own families. Thus, presenting North Carolinians, including those identifying as American Indian, with a ‘tobacco survey’ can sometimes elicit adverse feelings. Some potential respondents felt judgment from the survey specialists and/or academic research team. They perceived the survey was working against a vital component of tribal communities, both in the form of traditional tobacco use and the economic livelihood of commercial tobacco. When community members expressed these concerns at events, the survey specialists spent a great deal of time explaining the purpose of the survey. They clarified that asking about commercial tobacco use is not intended to cause offence or be a judgment toward anyone’s behaviour. Rather, completing the survey ensured tribal communities in North and South Carolina are represented in the data, which will enable better support and resource allocation in the future. Reframing the narrative to highlight the importance of elevating tribal voices often, but not always, led to participants agreeing to complete the survey. Building trust and rapport with potential respondents by listening to and addressing their concerns, especially related to the significance of tobacco, is a primary reason why more than 2500 American Indian adults completed the survey. Indeed, one tribe invited Ms Chavis to present at a community event even though historically people from other tribes do not attend. The trust the survey specialists achieved is also evident based on the number and breadth of events they attended (see Table 2).
Although the survey completion rate has far exceeded original expectations, recruitment challenges were still experienced. Initially, we intended to use social media and other online venues to advertise the survey during the winter months when fewer tribal community events are scheduled. However, given the challenges with survey-scammers that emerged without using online recruitment, we decided against sharing the survey on social media or other websites (further details given below). Unfortunately, without social media, our sample is primarily comprised of people attending tribal community events; therefore, it is possible those people do not necessarily represent all American Indian adults living in North or South Carolina. However, we felt this trade-off was necessary to ensure high quality data collection. Additionally, we determined that in some scenarios, large community events did not lead to substantial increases in survey respondents. We believe this is likely due to a combination of factors such as the location of the survey booths in low foot traffic areas, the number of competing activities (for example, dancing, pageants) occurring within the event schedule and poor weather conditions for outdoor venues (for example, dangerously high temperatures). Thus, for future surveys, large events will be important for survey awareness and community visibility of the research team, but may not be relied upon as a major recruitment opportunity.
For Catawba Nation, because it is located in South Carolina and therefore outside the North Carolina Commission of Indian Affairs’ jurisdiction, we had to use a different recruitment approach. Since we did not have the funds to hire another survey specialist to attend community events in South Carolina and we could not use social media, we worked with the Catawba Indian Nation Wellness Department to mail flyers directly to enrolled members of the Catawba Nation. We provided flyers and envelopes for up to 1000 respondents. The response to this approach was surprisingly effective. Within three weeks of the mailing, we had over 250 new Catawba Nation respondents. Given the relatively low cost and high return, we intend to use this same approach with tribes in North Carolina that we would like to see have more representation in future surveys. This will help to ensure the distribution of survey responses generally reflect the overall American Indian population in North Carolina.
Another important, albeit obvious, lesson learned was the need for tribal community member review and feedback on survey flyers and social media advertisements to ensure cultural relevance and appeal. Unfortunately, the original survey flyer, which required institutional review board approval from Wake Forest, was created quickly because the survey launch was imminently approaching. To facilitate speed, an advertisement from one of Dr Denlinger-Apte’s previous smoking studies was adapted (see Figure 4). However, the survey specialists received feedback during the first few community events that some individuals perceived the flyer as promoting commercial tobacco use since the image included cigarettes. We then amended the flyer to include an image of dried tobacco leaves (see Figure 5), which aligns with tribal culture and North Carolina as a tobacco-growing state.
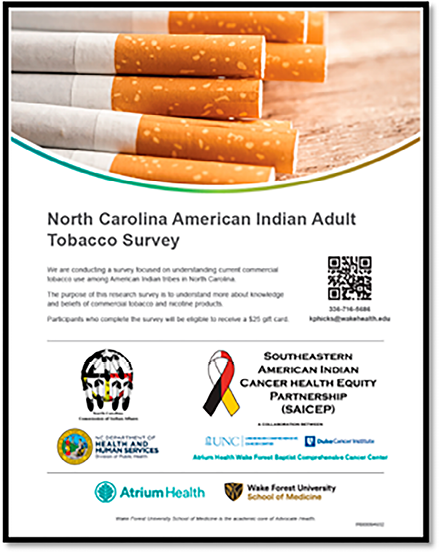
Figure 4. Original survey flyer
Figure 5. Revised survey flyer
Finally, from a practical standpoint, a key lesson learned is the need to balance the ease of responding to the survey with protection against survey bots and scammers. Because the primary method for survey recruitment was community-facing events, ease of survey completion while in the field was prioritised. We wanted people to feel as though they could easily complete the survey on their phone by scanning a Quick Response code while attending a community event or take home a flyer with a Quick Response code to complete later. We did not include Captcha’s or other bot-deterrent methods (for example, duplicate internet provider restrictions) due to concerns that it would make it harder for community members to complete the survey, especially for individuals with lower technological literacy. For the first few months of recruitment, this approach worked successfully. However, scammers eventually identified the survey as an opportunity to earn money, which led to multiple attacks by survey scammers. Because respondents receive $25 for survey completion, scammers were motivated to complete the survey multiple times to earn the incentive. To address the scammer attacks, we implemented several changes in REDCap both to deter bot completion of the survey and to assess the likelihood that answers were from real respondents versus scammers (for example, open-ended questions, decoy questions). Respondents provided their names and contact information so Wake Forest and the North Carolina Commission of Indian Affairs could mail participants their gift card incentives. This allowed our survey specialists from the North Carolina Commission of Indian Affairs and research staff from Wake Forest (Ms Darcy Lockhart, Ms Hicks and Ms Harwood) to contact each person who was eligible to receive a gift card to confirm they had participated in the survey. An Excel formula was developed to allow for objective review of particular survey items (that is, timestamp, eligibility criteria, blank responses to required questions) to evaluate the likelihood of a bot response. This formula was implemented in spring 2024; however, the North Carolina Commission of Indian Affairs and Wake Forest teams called all participants who provided their contact information to confirm survey completion in addition to utilisation of the Excel formula.
Conclusion
Multi-sector collaborations that include American Indian leaders, public health professionals and academic expertise along with partnership from three influential cancer centers in the state have been essential for ensuring the gap in data evaluating commercial tobacco use among American Indians in North and South Carolina is narrowed. Building trust with community members and across professional sectors has also been key for the success of this project.
References
American Lung Association 2024, New report: North Carolina must focus on increasing funding for tobacco control to save lives, https://www.lung.org/media/press-releases/north-carolina-2024-state-of-tobacco-control.
Bell, RA, Akinyemiju, T, Barrett, N, Denlinger-Apte, R, Wheeler, SB, Dial, R, Salas, A, Hunt, C, Raveendran, Y & Fennimore, E 2025, ‘Understanding and addressing cancer disparities among American Indians in North Carolina: The Southeastern American Indian Cancer Health Equity Partnership (SAICEP)’, Cancer Control, vol. 32. https://doi.org/10.1177/10732748251336410
Cornelius, ME, Loretan, CG, Wang, TW, Jamal, A & Homa, DM 2022, ‘Tobacco product use among adults – United States, 2020’, Morbidity and Mortality Weekly Report, vol. 71, no. 11, pp. 397–405. https://doi.org/10.15585/mmwr.mm7111a1
D’Silva, J, O’Gara, E & Villaluz, NT 2018, ‘Tobacco industry misappropriation of American Indian culture and traditional tobacco’, Tobacco Control, vol. 27, no. e1, pp. e57–e64. https://doi.org/10.1136/tobaccocontrol-2017-053950
Daley, CM, Greiner, KA, Nazir, N, Daley, SM, Solomon, CL, Braiuca, SL & Choi, WS 2010, ‘All nations breath of life: Using community-based participatory research to address health disparities in cigarette smoking among American Indians’, Ethnicity & Disease, vol. 20, no. 4, pp. 334–38.
Henderson, PN, Lee, JP, Soto, C, O’Leary, R, Rutan, E, D’Silva, J, Waa, A & Henderson, ZP 2022, ‘Decolonization of tobacco in Indigenous communities of Turtle Island (North America)’, Nicotine & Tobaco Research, vol. 24, no. 2, pp. 289–91. https://doi.org/10.1093/ntr/ntab180
Irby, MB, Ballard, PJ, Locklear, T, Jeffries-Logan, V, Brewington, T, Byrd, R & Bell, R 2021, ‘Native pathways to health: A culturally grounded and asset-based CBPR project exploring the health of North Carolina’s American Indian communities’, North Carolina Medical Journal, vol. 82, no. 6, pp. 398–405. https://doi.org/10.18043/ncm.82.6.398
Lempert, LK & Glantz, SA 2019, ‘Tobacco industry promotional strategies targeting American Indians/Alaska Natives and exploiting tribal sovereignty’, Nicotine & Tobacco Research, vol. 21, no. 7, pp. 940–48. https://doi.org/10.1093/ntr/nty048
McCraw, L 2023, The history and significance of sacred tobacco for American Indians, https://www.dukeunctts.com/post/the-history-and-significance-of-sacred-tobacco-for-american-indians.
North Carolina Department of Health and Human Services 2021, Smoking and COVID-19, https://tobaccopreventionandcontrol.dph.ncdhhs.gov/Documents/SmokingandCOVID19-WEB.pdf.
Shahbandeh, M 2024, Leading tobacco producing U.S. states from 2021 to 2023 (in 1000 pounds), https://www.statista.com/statistics/192022/top-10-tobacco-producing-us-states/#:~:text=North%20Carolina%20lies%20in%20the,and%20starts%20around%2018%20years.
US Department of Health and Human Services 2014, The health consequences of smoking – 50 years of progress: A report of the Surgeon General, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, https://www.hhs.gov/sites/default/files/consequences-smoking-exec-summary.pdf.
US Food and Drug Administration 2023, Commercial tobacco use in American Indian and Alaska Native populations, https://www.fda.gov/consumers/health-education-resources/commercial-tobacco-use-american-indian-and-alaska-native-populations.