Gateways: International Journal of Community Research and Engagement
Vol. 19, No. 1
March 2026
PRACTICE-BASED ARTICLE
Embedding Research in Infant and Early Childhood Mental Health Settings: Practical Steps and Considerations
Lamia Firasta1,3,†, Evelyn Chan2,†, Mary Motz1, Samantha Kempe3, Naomi Andrews4, Bhupinder Heer1, Denise Penaloza2, Shainur Premji5, Nancy Poole6, Hannah McDowell3, Debra Pepler7,‡, Nicole Racine3,8,*,‡
1 Mothercraft Breaking the Cycle, 393 King St. East, Toronto, Ontario
2 Maxxine Wright Community Health Centre, Fraser Health Authority, 13733 92 Ave, Surrey, British Columbia
3 School of Psychology, University of Ottawa, 136 Jacques-Lussier, Ottawa, Ontario
4 Department of Child and Youth Studies, Brock University, 1812 Sir Isaac Brock Way, St. Catherines, Ontario
5 Centre for Health Economics, University of York, Heslington, York YO10 5DD, United Kingdom
6 Centre of Excellence for Women’s Health, Vancouver, British Columbia
7 Faculty of Health, Department of Psychology, York University, 4700 Keele St, North York, Ontario
8 Children’s Hospital of Eastern Ontario Research Institute, Ottawa, Ontario
† Represents shared first authorship
‡ Represents shared senior authorship
Corresponding author: Nicole Racine, nracine2@uottawa.ca
DOI: https://doi.org/10.5130/wbjs1p29
Article History: Received 01/04/2024; Revised 22/11/2025; Accepted 04/12/2025; Published 03/2026
Abstract
Evidence-based programs that address the mental health needs of infants and young children exposed to early adversity are essential for disrupting patterns of intergenerational risk. There is now a growing understanding that research must be co-created in collaboration with community partners, as research and evaluation are both core components of implementing infant and early childhood mental health programs. Yet less than half of infant and early childhood mental health programs in Canada have research and evaluation embedded within their core services. Embedding evaluations within a mental health program requires trust, relational development and the use of frameworks and methods that meet the needs of the program.
The process of embedding research within a community program setting has the potential to inform program improvements, provide critical information to funders and build evaluation capacity within the field of infant and early childhood mental health. This article provides a road map from the perspectives of embedded research staff, on-site service providers and academic researchers for conducting community-based research (CBR) within infant and early childhood mental health settings.
First, we provide a conceptual foundation of CBR along with an explanation of how these concepts can be applied within programs delivering infant and early childhood mental health services. Next, we detail and compare the histories of two community-based interventions for pregnant and parenting substance-involved mothers and their families: Breaking the Cycle (BTC), a program which has had research embedded within its operation from the onset and Maxxine Wright Community Health Centre (MWCHC), a similar program in the early stages of embedding research. We detail how an established researcher-community partnership served as a model for the second collaboration. Specifically, we describe how a community-based researcher (the ‘research person’) can function as a bridge in facilitating community-university partnerships. We highlight specific strategies and considerations for clinicians and researchers interested in building community research partnerships. Moreover, we provide practical guidance for embedding CBR within their programs to support relational approaches and research sustainability. Finally, we discuss collective reflections for increasing the uptake of infant mental health research and research practices in Canada.
Keywords
Community-based Research; Community Psychology; Infant Mental Health Services; Research; Evaluation; Community–University Partnerships
Introduction
Research practices and methods continuously evolve to meet the complexities of modern challenges. One approach that has existed for decades and has gained traction within the field of mental health is community-based research (CBR) (Nelson, Lavoie & Mitchell 2007). CBR is recognised as a research method and framework that promotes engagement, co-creation and collaboration between researchers and community partners. Specifically, these research methods aim to shift the narrative from ‘conducting research on’ to ‘conducting research with’ (Malone 2024; Mankowski, Galvez & Glass 2010; Turnbull, Friesen & Ramirez 1998).
Within a community research framework, research practices are embedded within the community setting rather than ‘parachuted in’ solely for data collection purposes (Pepler 2016). Instead, embedded community-researchers enter the community environment and integrate into the routine operations of the community program, acting as intermediaries between research practices and clinical operations. This approach allows researchers to foster trust and ensure safety in their relationships with the staff and service users (Israel et al. 1998). Although there are several descriptions of CBR theory and practice (Collins et al. 2018; Nelson, Lavoie & Mitchell 2007; Wallerstein 2021), and broad guidelines for establishing academic-community partnerships (Dolata, Collins & Nonguierma 2020; Saleh et al. 2022), there is limited literature that provides tangible strategies on how to integrate and engage research within community-based programs successfully, particularly in infant and children’s mental health settings.
It is crucial to document effective strategies for integrating research into community settings that serve vulnerable populations; documentation of said strategies helps ensure that research and clinical practices are conducted with sensitivity and respect for the participants. Enhancing knowledge on the process of embedding research practice, especially in infant and child mental health community settings, has the potential to inform practices within community organisations that wish to build research capacity to support their evaluation outcomes.
The purpose of this article is to provide a road map for establishing a community-university partnership within infant and early childhood mental health settings.This article, written from the perspectives of embedded community-based researchers, on-site service providers and academic researchers, outlines components and steps to guide the implementation of a community-based research process within organisations providing services to children and families. We begin by providing a conceptual foundation of CBR and explaining how CBR can be applied within programs delivering infant and early childhood mental health services.
Next, we describe how Breaking the Cycle (BTC), a program with over 30 years of embedded research, has supported academic collaborations from multiple institutions, and how this foundation informed the integration of a CBR protocol and researcher at a new site, Maxxine Wright Community Health Centre (MWCHC), as a part of a community-university partnership with the University of Ottawa.
We highlight strategies and considerations for clinicians and researchers interested in embedding data collection, evaluation and best research practices for effective community engagement within their programs. Finally, we discuss future directions for increasing the uptake of infant mental health research and research practices in Canada.
Background on CBR
CBR involves a collaborative approach with non-academic partners to co-create knowledge that leads to sustainable social change (Israel et al.1998; Minkler et al. 2012). Within a CBR framework, a research partner, typically researchers who are housed at an academic institution, will collaborate with a community-based organisation, health centre, or not-for profit, to develop research aims and goals jointly (Springer & Skolarus 2019). Emphasis is placed on mutual learning in which the knowledge and skills of the research partner are used to address research questions that align with community partner expertise, feedback and curiosity (Reed 2015).
The central values of collaboration, equitable partnerships, knowledge sharing, learning and action comprise the heart of CBR (Ozano et al. 2024). Barbara Israel and colleagues (1998) identified several overarching principles to consider when integrating CBR into a community-based organisation including the importance of steady communication, building on existing community resources and strength and acknowledging the unique identity of the community. Partner and researcher readiness, safety, competence and collaboration have been highlighted as essential components of CBR (Andrews et al. 2021). To be precise, researchers should assess the readiness of organisations in advance, receive sufficient training on safe study execution and adopt a humble and collaborative stance.
CBR within infant and child mental health settings
Over the last 30 years, evidence on the use of CBR approaches in the field of infant and childhood mental health has emerged (Bondi, Leslie & Motz 2023; MacDonald et al. 2019; Rodríguez et al. 2018). CBR approaches are well suited to infant and childhood mental health settings for several reasons. First, infant and childhood mental health programs are often required to undertake research and evaluation as part of funding mandates. Secondly, mental health clinicians and practitioners are central to the development and delivery of mental health services and have expertise that can inform the research process and outcomes. Thirdly, relational development, creating trusting relationships, is a core process of both CBR and infant and mental health. Taken together, CBR approaches can lend themselves well to the research and evaluation needs of infant and childhood mental health settings (Israel et al. 1998).
Despite the need for evaluation of programs that provide services to infants, children and their families, very few community-based settings in infant and child mental health have integrated a research evaluation component into their services (Racine et al. 2022; Yoon, Snyder & Yoon 2020). Furthermore, although previous research does provide strategies, theoretical foundations and models for CBR (Andrews et al. 2021; Pepler 2016; Racine et al. 2022) and community-academic partnerships (Dolata, Collins & Nonguierma 2020; Saleh et al. 2022), to our knowledge, there remains a lack of comprehensive guidelines on how to embed researchers and implement research partnerships within community-based organisations, specifically in the context of infant and child mental health.
Below we provide an overview of the different services and approaches used at two early-intervention programs, BTC and MWCHC, to contextualise their purpose in a collaborative research project alongside the University of Ottawa, the academic partner. We highlight how methods for conducting CBR within BTC, which has research woven into its core operations, were used to inform the integration of similar research practices and principles in MWCHC.
Breaking the Cycle program (BTC)
Established in 1995 with the Canadian Mothercraft Society, BTC is an early intervention and prevention program in Toronto, Canada for substance-involved pregnant people1 and parenting mothers, as well as their young children under the age of six (Leslie 2011; Motz et al. 2006; Motz, Reynolds & Leslie 2020; Pepler et al. 2002, 2014). The program was established to support the development of infants and children exposed to substances by addressing maternal substance use and the co-occurring challenges and contextual risk factors (for example, trauma, violence, social inequality) (Bondi et al. 2021).
Prior to the development of BTC, service delivery for substance-involved pregnant people and mothers was often fragmented across adult and child services sectors, such as women’s addiction and health services and child welfare and child development services. To tackle this gap, BTC services simultaneously support mothers to address maternal substance use, mental health challenges and past trauma, alongside their children’s development and wellbeing.
BTC offers a wrap-around model of services where families can receive a variety of supports in one location. Specifically, services offered include parenting interventions (for example, Circle of Security Parenting Group (Hoffman et al. 2006), New Mom’s Support Group, Parent-Child Mother Goose Program), individual and group addiction counselling (for example, Relapse prevention, Life skills group), developmental screening and assessments, child-care, early childhood interventions, basic needs support and interpersonal violence interventions (for example, Connections group (Pepler et al. 2014)).
Services are delivered through a partnership model which involves representation from several sectors spanning mental health, public health, probation and parole and child welfare and children developmental services, all of which have long been proven effective (Motz et al. 2006; Pepler et al. 2014). In addition to core services provided in the centre, home visitations and a pregnancy outreach program provide services to families within the prenatal period (Leslie 2011). Given that the mother-child relationship is a central determinant of child development (Leslie 2011; Motz et al. 2006), the program uses developmental-relational approaches and evidence-based interventions (Andrews et al. 2019) to assist mothers in developing consistent, safe and nurturing parenting behaviours. This in turn supports the development of a healthy attachment relationship.
To sustain the work done at the centre, BTC must continue to meet periodic funding mandates and assessments of fund allocation in relation to program effectiveness. As a result, from inception, BTC has embedded research within its programming to measure and demonstrate ongoing program impact. This integrated approach was feasible as the centre already had a trained clinical psychologist and researcher clinician on-site who could assist with incorporating data collection into daily operations. To supplement program evaluation further, BTC established partnerships with academic institutions to better characterise the mothers who were accessing services and measure maternal-infant outcomes. Researchers from these institutions were included in early program planning meetings to develop an evaluation framework and to ensure outcome assessments were an integral part of service delivery.
Over time, the research program has evolved to address the changing needs of the community and the increasing complexity of BTC’s services. With the support of grant funding, research at the centre has become more robust, expanding from descriptive designs to intervention-focused studies. To support this growth, the staff at BTC has expanded to include additional researchers, such as graduate students and research assistants, who assist in the integration of research practice and service delivery. Furthermore, over the last 30 years, through ongoing collaboration and co-creation between staff at BTC and researchers at academic institutions, knowledge from these program evaluations have been disseminated widely across Canada, informing the creation of new community and evidence-based interventions.
From program evaluations to academic research partnerships
BTC staff members have written many evaluation reports alongside academic partners to describe the outcomes of mothers and children involved in programming (Leslie 2011; Motz et al. 2006; Motz, Reynolds & Leslie 2020; Pepler et al. 2002, 2014). In a 2008 collaboration with York University, Canada, BTC was successful in securing funding to formally evaluate the outcomes of mothers engaged in the BTC program compared to those in another community program. Results from the study showed that supporting mothers in learning about and enhancing their relationships with their children through substance-use treatment was linked with positive changes in their substance-use and improvements in their mental health symptoms (Pepler et al. 2014).
Since then, collaborators have continued to be interested in evaluating the effectiveness of BTC services in promoting child development. The University of Ottawa is one such key collaborator, and through this strong, ongoing partnership, BTC has strengthened its embedded research capacity and created opportunities to expand these studies to other sites serving similar populations. During a previous collaboration on services and outcomes of wrap-around programs across Canada for at-risk pregnant and parenting mothers (Rutman et al. 2020), staff at BTC first developed a relationship with staff at MWCHC in Surrey, British Columbia. Building on this collaboration, the two sites established a research partnership to study, assess and compare the developmental outcomes of children involved in BTC and MWCHC. The current project is an extension of this work, with a focus on child outcomes and the mother-child relationship.
Maxxine Wright Community Health Centre (MWCHC)
Since 2005, MWCHC has provided integrated health and social services for mothers who are impacted by substance use, domestic violence and/or historical cultural violence (Robinson et al. 2003). The centre intakes clients who are pregnant or who have a newborn under six months. These families may continue to access services until the youngest child enters school. Delivered by a multi-disciplinary team, these services include primary health care in the form of prenatal, postnatal, mental health and substance use care, as well as other supports such as counselling, case management, dental hygiene and referral, parenting groups, activity groups, a food program and access to household and clothing donations.
MWCHC is operated in a partnership with Fraser Health Authority, Atira Women’s Resource Society and the British Columbia Ministry for Children and Family Development (Atira Women’s Resource Society n.d.). The centre’s approach to care is women-centred and focuses on harm reduction, ensuring that trauma informed values guide all care and services. Having recently joined the Indigenous Health sector of Fraser Health, MWCHC has been working on implementing Indigenous cultural practices and support. MWCHC’s current approach to care is mother-centred, with children typically being given primary health care in the form of health treatments and immunisations.
Through their partner organisation, Atira Women’s Resource Society, MWCHC also offers housing for mothers with infants up to six months, and a second stage residence where mothers and their children can stay for two years. MWCHC has previously collaborated with researchers as part of individual research projects and has conducted their own internal evaluations; however, a large-scale and long-term research project has never been embedded. MWCHC is funded by Fraser Health Authority, a publicly funded health service provider. Accordingly, MWCHC gathers data on service utilisation, reporting the number of clients and the types of services accessed within a given period. Unlike BTC, there has never been a need to demonstrate MWCHC’s service effectiveness and impact through ongoing embedded research.
The goal in implementing CBR practices at MWCHC is to collaborate directly with the community, to gain insight into the effectiveness of current services and to learn best practice methods of infant mental health care and mother-child relationship building alongside BTC. The current partnership between BTC and MWCHC, the Early Relationships Study (ER Study), is an extension of BTC’s previous collaborative work and will identify strategies for implementing a relationship-oriented approach in care for substance-involved mothers and their young children, which in turn may interrupt intergenerational patterns of trauma and substance use (Espinet et al. 2016).
The Early Relationships Study (ER Study)
The ER Study is a longitudinal study examining the developmental outcomes of infants and young children at BTC and MWCHC, coordinated by researchers from the University of Ottawa (Racine et al. 2024). The goal is to understand what support and services are most effective in optimising the developmental and mental health outcomes of infants and young children in contexts of risk. In particular, the ER Study examines whether relational, mother-child centred models of care enhance the dyad relationship and improve long-term child developmental outcomes. BTC partnered with MWCHC, to evaluate and describe two models of care.
Moreover, the project aims to understand the mechanisms of change within each program. As part of the study, mothers complete questionnaires about their background, maternal mental health, views on parenthood, parenting style, as well as their child’s development. Parental sensitivity is assessed through a video recorded play interaction between mothers and their children. These measures are conducted longitudinally, following the mother-child dyad for up to three years. Overall, the ER Study aims to identify effective methods for strengthening the mother-child relationship among women living in vulnerable contexts of substance use or violence.
Funding context
The ER Study is funded by the Canadian Institute of Health Research (CIHR) via a federal call for early intervention, implementation science projects as part of the Mental Health in the Early Years Team Grant Competition. Having both BTC and MWCHC partnered with the University of Ottawa was central to advancing the ER Study, as academic involvement is required to secure CIHR funding. Therefore, prior to grant submission, the University of Ottawa collaborated closely with the two sites, while simultaneously securing letters of support from organisations and involved parties.
The grant funding ultimately allowed the team to hire full-time embedded researchers at both sites, though the hiring process differed. At BTC, the researcher was hired as a University of Ottawa employee, while at MWCHC, the researcher was hired directly under the health authority. This distinction reflects site-specific technological access, varying degrees of team integration and community-partner preference.
The process of integrating research into a community-based organisation
When embedding research into infant and childhood mental health programs, it is essential to have a pre-existing relationship with the potential partner organisation. Staff at BTC and MWCMC had previously collaborated on a separate research project with an external organisation, hence they had a shared understanding of the approaches used at each site, along with a willingness and openness of collaboration, shared decision making and shared benefits (Rutman et al. 2020). Described below is the process of embedding and engaging research practices at MWCMC using the approaches developed over decades at BTC. A summary of the steps that were used for implementation can be found in Figure 1.
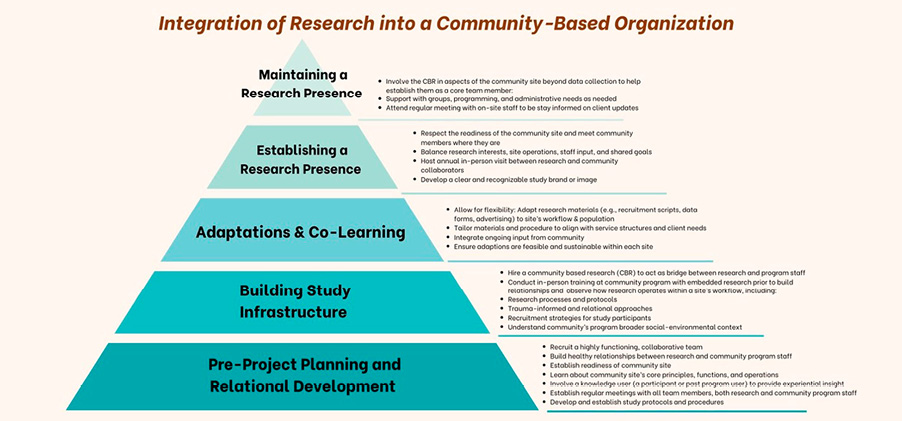
Figure 1. Framework detailing the process of CBR integration within an organization, focusing on phases of relationship development, infrastructure building, co-learning, and the establishment and maintenance of a research presence.
Pre-project planning and relational development
Building healthy relationships between researchers and community program staff is a core requirement for integration of research into a second site; a highly functioning team is critical in supporting this process. Through trusting relationships, a site can establish capacity and feasibility. To establish trust, it is important to first learn about the core values, functions and operations of an organisation. Additionally, the program must value the proposed research, ensuring that adequate resources are allocated for the project (for example, funding, space and staff time).
Once readiness is established, emphasis can be placed on continuing to develop the research relationship through joint meetings to co-create the goals and methods for the research project. As part of this process, having input from a knowledge user, someone who has participated in the program in the past, can inform the researchers on community priorities that reflect the realities of those with lived experience.
An important output from this step is the development of the study protocol and subsequent approval from the appropriate research ethics board. While this phase of the project can take several months and may require several meetings, it can be expedited if researchers are already familiar with a community organisation or have a pre-established relationship with them through another project.
Building study infrastructures
Several steps are required to support the integration of research infrastructure into a community-based organisation. One of the most important steps involves hiring appropriate research staff. Previous research shows that a person directly responsible for implementing the study protocol, including participant recruitment, data collection and data entry (referred to as ‘the research person’) is crucial for research success (Pepler et al. 2014). The role of the research person involves implementing and maintaining CBR practices within the organisation while acting as a bridge between all team members involved in the project. In addition to having a strong background in research processes and program management, the research person must have strong relational skills and be other-oriented (Skipper & Pepler 2020); that is, they must integrate into the processes and culture of the community organisation where they are working through fostering relationships with clients and staff. The research person may be asked to take on roles to support the functions of the community organisation and build relationships. For example, at MWCHC, the research person worked with a staff member to co-facilitate a social group for mothers. This allowed the research person to become familiar with the staff and clients at the site and to learn about their services.
To further build a research framework at a specific site and build robust relationships, it is helpful to have an initial, in-person meeting. For the ER Study, three staff members from MWCHC were invited to the BTC site for training, providing them with the opportunity to observe study processes and protocols, and the ways relational and embedded research approaches shape the centre’s workflow and programming. This visit helped inform the MWCHC staff on how CBR operates and functions within a clinical setting. Staff from MWCHC also had the opportunity to learn about trauma-informed and relational approaches to research, including strategies for advertising and recruiting mothers into the study. With firsthand knowledge and expertise gained during the visit, it was relatively easy to develop and establish study protocols and procedures suitable for MWCHC. Various virtual meetings were held from then on to facilitate ongoing relationship development, training of research staff and data monitoring (Fecher et al. 2021).
In addition, a strong understanding of a program’s broader social-environmental context is crucial in establishing an effective community-university partnership. For example, one program could experience a particular governmental or funding climate that impacts service delivery, and in turn, affects research outcomes. Taking these shifts into consideration, University of Ottawa conducts bi-annual interviews with staff at the two study sites to understand the circumstances and changes in which the programs are operating. Moving forward, it is expected that these interviews will provide context to the findings, further enhancing understanding of outcomes.
Adaptation and co-learning
As the target population served may vary across organisations, it is important to allow for flexibility and continuous integration of community partner input when conducting CBR. Study procedural materials (that is, recruitment scripts, advertising materials, data tracking sheets, data entry sheets) can be developed in advance, however, they may need to be adapted to fit the needs of specific programs. For example, at MWCHC, the clients first meet with a nurse practitioner to assess what services would suit them best, whereas at BTC, clients meet with the Program Manager initially, before being transferred to the Addictions Counsellors and Parent-Infant Therapist. When introducing the ER research protocols at MWCHC, the staff needed time to discuss and consider how best to implement the research protocols while maintaining regular workflow.
Understanding client engagement with services is important for both research recruitment and follow-up. With study recruitment at MWCHC for instance, mothers were less likely to learn about the research through posters and flyers in the centre. As a result, it was decided that the public health nurses would directly facilitate an in-person introduction to the study with the clients; they are already familiar with the client and have the capacity in their schedule to assist with recruitment, unlike the other healthcare professionals at the centre. Other site-specific adaptations to the protocol at MWCHC include the use of a visual tool when delivering feedback to parents on developmental outcomes, rather than through a formal report and administering a different set of mental health measures compared to BTC to match those that were delivered clinically. These adaptations helped to increase acceptability and feasibility of research implementation at MWCHC.
Establishing a research presence
Having already developed research foundations through a robust study infrastructure and strong relationships with the site staff, it is essential to continue embodying readiness, safety, competency and collaboration during participant recruitment and beyond. The key to establishing a research presence involves clear communication, building rapport with staff and participants and encouraging study engagement. Through these efforts, the research persons can integrate themselves in a program as trusted members of the team.
The first crucial step when working with staff at a new site is to meet them where they are at. Researchers must consider the familiarity and comfort of staff members with research processes, then work alongside them to engage, identify and recruit participants into the study. Additionally, researchers should respect the centre’s workflow and workload, while actively incorporating staff feedback into the study design. In developing the recruitment process at MWCHC, for example, the research person collaborated with the on-site staff to ensure all procedures aligned with the centre’s operations.
As the study progresses, the research person continues to serve as a mediator to balance research interests with the practicalities of on-site operations and input from on-site staff. In another effort to create a solid research presence and foster successful research relationships, select members of the research team pay annual visits to both MWCHC and BTC. The on-site investigator, staff clinical psychologist and the primary investigator visit MWCHC in-person to provide study updates to the on-site MWCHC team, to better understand current circumstances at the centre, and engage in discussions on shared goals for research implementation. In turn, the MWCHC research person and primary investigator visit BTC for a similar update meeting. These annual visits also establish a relational approach beyond the research component; in holding space for connection through shared meals, both groups are able to establish a bond apart from work. Personal relationships help in maintaining regular communication with management and site leads throughout the entire project.
Lastly, to establish a research presence, it is helpful to create an identifiable brand for the study. This can be achieved by having a recognisable image or logo placed around the site and on research-related materials. For the present research study, a stuffed toy mascot with the ER logo was given to participating mothers. This tangible keepsake serves as a reminder to participants of the research and the commitment of the research team in supporting them. In all, establishing a robust research presence through engaging with site staff, facilitating on-site interactions and developing study branding are needed for effective integration into the secondary site.
Maintaining a research presence
Maintaining research goes beyond collecting follow-up data through relational approaches with staff and families. It involves integrating research protocols and the research persons themselves as core components of program functioning. This approach places the research persons in a unique position to contribute beyond a research capacity by actively supporting and participating in various initiatives within the centre.
Through integration, the research persons can form connections with the clients and staff and deepen their understanding of community strengths, needs and challenges. A key way the research person maintains a research presence beyond data collection is through regular communication with the participants. For instance, both the research persons at BTC and MWCHC create seasonal newsletters for the ER Study, which helps them keep participants and staff informed on broad study updates and happenings around the centre. Additionally, their responsibilities may include assisting with activity groups, programs and administrative tasks, all of which contribute to the centre’s overall operations. In this way, research persons can act as a bridge between research and clinical practice, centring themselves as members of the community. Involvement in programming beyond the research role can look different depending on the program. At MWCHC, the research person participates in programs such as the Just for Fun activities group, Rhyme Time nursey rhyme group, cooking classes and Circle of Security parenting group (Hoffman et al. 2006). When mothers had appointments at MWCHC, the research person would often offer to hold their babies or watch over their children, providing another means of hands-on support. At BTC, the research person assists in covering reception, helping cook in the kitchen, assisting in the playroom, as well as holding babies, assisting in warming up milk, gathering and cooking food and snacks during the research recruitment process or after the mother-child play activity.
Every morning, staff at each site participate in a daily huddle to discuss new clients, stay updated on the ongoing programming and review scheduled appointments. In addition, the research person attends monthly administrative meetings to discuss updates from staff on clients, program planning, new referrals, case closure and research updates. By engaging in aspects beyond formal research at the sites, the research persons become recognisable staff members and trusted faces, ultimately fostering rapport and trust within the community through relationships.
Navigating barriers and mitigation strategies when embedding research
Barriers inevitably arise in the process of conducting CBR. If some of these barriers can be anticipated, mitigation strategies can be developed to reduce their impact. While there is no single way to address barriers in CBR, we prioritise a relational approach to balance what is ideal and what is practical in real-world settings (Reed 2015).
Physical distance
A common barrier in CBR is maintaining clear and consistent communication with all collaborating organisations. Effective communication strategies are crucial in the current study for ensuring all partner organisations and researchers across several locations are informed and aligned. To address this challenge, the research team implemented multiple communication strategies with technology-facilitated online meetings to provide regular check ins and updates among various team members, as well as occasional in-person meetings for continued relationship building. In particular, the research persons attend bi-weekly updates on the ER Study with collaborators and weekly meetings with a university-based clinical research coordinator, both held online. Once a year, members of the research team will visit the BTC and MWCHC sites to present study progress and preliminary results, while encouraging feedback and input from on-site staff. Continuous, direct communication in various forms ensures that all research collaborators are well informed on study updates and that research practices stay aligned with the needs and goals of everyone involved.
Staff changes and turnovers
Staff turnover in CBR can be challenging, given the need for incoming staff to build connections and trust within the community (Pascoe et al. 2021). As such, changes in staff can slow study progress. In the ER Study, the initial research person hired at MWCHC left the position after nine months. However, several strategies were implemented prior to the staff change, to ensure knowledge transfer, retention and a smooth role transition.
For example, to promote continuity in the ER Study, the research person at MWCHC created a standard operating procedure document, which outlines detailed steps, notes and processes pertaining to their role. This guide contains practical information on study procedures, as well as resources ranging from best recruitment practices to data collection file access. Maintaining an updated guide is crucial to ensuring that future staff have a clear understanding of their responsibilities from the onset.
In addition, a process was implemented for the research person to maintain a journal to provide informal documentation of day-to-day happenings, observations and activities at the centre. In contrast to the standard operating procedure, the journal captures insights from the community as well as lessons learned through direct interactions. This documentation helps incoming staff to learn the daily expectations of the position and the nuances at the site.
Finally, it is helpful to have overlapping time between outgoing and incoming staff members. At MWCHC, this time allowed the new research person to ease into the role. Direct knowledge transfer during this training period allowed the new research person to ask questions and establish connections in the community through the existing ones made by the previous research person.
Client challenges
Since CBR is situated in a real-world setting, it is important to be considerate of client challenges when adhering to research protocols for recruitment, data collection and follow-ups (Wallace et al. 2015). Good judgment and a willingness to adapt is needed when recruiting participants from vulnerable populations. Often, the clients basic needs are not being met or their living situations may be precarious, which could include circumstances such as unstable housing or interpersonal violence. Therefore, it is crucial that the research person and site staff work collaboratively to allow for flexibility in the study timeline and procedures.
The research persons should follow the judgement of clinicians during recruitment and follow-ups to create trauma-informed and sensitive procedures for approaching clients. As such, participants are made aware that there is no need to sign up for the study immediately, and if they have any concerns or questions, the research person is always available to check-in with them. Taking client challenges into account requires sensitivity; although trained researchers, there is still a need for the research persons to familiarise themselves with the clients and their living situations while developing their clinical research judgement. The research persons must also know when to defer to the expertise of on-site staff and how to effectively collaborate with their team to achieve study progression.
Conclusion
The co-production of research practice between community organisations and academic partners can generate new knowledge that can inform program development and planning. Through the experiences of collaborative research over the last 30 years at BTC, these developed processes and strategies guide the extension and implementation of its research program to other community-based organisations. Leading with community-centred and relational approaches has made it possible to develop strong collaborations with other community-based organisations. Importantly, research has been implemented in ways that are acceptable, feasible and effective.
The role of embedded research persons is integral to the successful implementation of research. The ability and willingness of the research persons to develop strong relationships, be flexible in their processes and approaches, participate in activities beyond the traditional research job description and maintain strong communication with multiple team members is imperative. Moving forward in CBR across multiple settings, it is important to learn from previous collaborative work. Continued collaboration will be directed towards generating and disseminating research evidence that enhances service provision for mothers and their infants and young children living in vulnerable contexts.
References
Andrews, N, Motz, M, Bondi, BC, Leslie, M & Pepler, DJ 2019, ‘Using a developmental-relational approach to understand the impact of interpersonal violence in women who struggle with substance use’, International Journal of Environmental Research and Public Health, vol. 16, no. 23, p. 4861. https://doi.org/10.3390/ijerph16234861
Andrews, N, Reynolds, W, Leslie, M, Motz, M, Zuberi, S, Singh, C & Pepler, DJ 2021, Building connections for healthy relationships: What we learned, Mothercraft Press, https://www.kh-cdc.ca/en/project-profiles/pdfs/Building-Connections-Plain-Language-Report-ENG.pdf
Atira Women’s Resource Society n.d., Maxxine Wright Community Health Centre, viewed 11 March 2025, https://atira.bc.ca/what-we-do/program/maxxine-wright-community-health-centre/
Bondi, BC, Leslie, M & Motz, M 2023, ‘Breaking the Cycle: Applying a partnership-based, three-client, early intervention model within a child welfare framework to care for children exposed prenatally to substances’, Child Welfare, vol. 101, no. 3, pp. 107–40. https://www.jstor.org/stable/48752732
Bondi, BC, Pepler, DJ, Motz, M & Andrews, N 2021, ‘Cumulative risk, protection, and early intervention: Neurodevelopment in sibling groups exposed prenatally to substances’, Developmental Neuropsychology, vol. 46, no. 7, pp. 498–517. https://doi.org/10.1080/87565641.2021.1986044
Collins, SE, Clifasefi, SL, Stanton, J, Straits, KJE, Espinosa, PR, Andrasik, MP, Miller, KA, Orfaly, VE, Gil-Kashiwabara, E, Nicasio, AV, Hawes, SM, Nelson, LA, Duran, BM & Wallerstein, N 2018, ‘Community-based participatory research (CBPR): Towards equitable involvement of community in psychology research’, The American Psychologist, vol. 73, no. 7, pp. 884–98. https://doi.org/10.1037/amp0000167
Dolata, J, Collins, C & Nonguierma, E 2020, B.R.A.C.E. Online toolkit: Building research for academic & community equity, https://cheeer.org/brace-toolkit/
Espinet, SD, Motz, M, Jeong, JJ, Jenkins, JM & Pepler, D 2016, ‘“Breaking the Cycle” of maternal substance use through relationships: A comparison of integrated approaches’, Addiction Research & Theory, vol. 24, no. 5, pp. 375–88. https://doi.org/10.3109/16066359.2016.1140148
Fecher, B, Kahn, R, Sokolovska, N, Völker, T & Nebe, P 2021, ‘Making a research infrastructure: Conditions and strategies to transform a service into an infrastructure’, Science and Public Policy, vol. 48, no. 4, pp. 499–507. https://doi.org/10.1093/scipol/scab026
Hoffman, KT, Marvin, RS, Cooper, G & Powell, B 2006, ‘Changing toddlers’ and preschoolers’ attachment classifications: The circle of security intervention’, Journal of Consulting and Clinical Psychology, vol. 74, no. 6, pp. 1017–26. https://doi.org/10.1037/0022-006X.74.6.1017
Israel, BA, Schulz, AJ, Parker, EA & Becker, AB 1998, ‘Review of community-based research: Assessing partnership approaches to improve public health’, Annual Review of Public Health, vol. 19, no. 1, pp. 173–202. https://doi.org/10.1146/annurev.publhealth.19.1.173
Leslie, M (ed) 2011, The BTC compendium: The roots of relationship, Mothercraft Press.
Malone, M 2024, Writing research differently: How community-university partnerships re-imagine the research article, Cambridge Scholars Publishing, Newcastle upon Tyne, UK.
Mankowski, ES, Galvez, G & Glass, N 2010, ‘Interdisciplinary linkage of community psychology and cross‐cultural psychology: History, values, and an illustrative research and action project on intimate partner violence’, American Journal of Community Psychology, vol. 47, no. 1–2, pp. 127–43. https://doi.org/10.1007/s10464-010-9377-y
McDonald SW, Madigan S, Racine N, Benzies K, Tomfohr L & Tough, S 2019, ‘Maternal adverse childhood experiences, mental health, and child behaviour at age 3: The all our families community cohort study’, Preventive Medicine, vol. 118, pp. 286–294. https://doi.org/10.1016/j.ypmed.2018.11.013
Minkler, M, Garcia, A, Rubin, V & Wallerstein, N 2012, Community-based participatory research: A strategy for building healthy communities and promoting health through policy change, PolicyLink.
Motz, M, Leslie, M, Pepler, DJ, Moore, TE & Freeman, PA 2006, ‘Breaking the Cycle: Measures of progress 1995–2005’, Journal of FAS International, vol. 4, no. 22.
Motz, M, Reynolds, W & Leslie, M 2020, The Breaking the Cycle compendium, volume 2: Healing through relationships, Mothercraft Press, Toronto.
Nelson, G, Lavoie, F & Mitchell, T 2007, ‘The history and theories of community psychology in Canada’, in SM Reich, M Riemer, I Prilleltensky & M Montero (eds), International Community Psychology, Springer US, Boston, MA.
Ozano, K, Alam, W, Aktar, B, Okoth, L, Chumo, I, Quach, JA, Muturi, N, Saidu, S, Gandi, I, Georgi, NW, Otiso, L, Conteh, A, Theobald, S, Dean, L, Tolhurst, R, Karuga, R, Karki, J, Garimella, S, Rao, V, Mwanki, A, Islam, N, Tengbe, SM, Dash, S, Saligram, PS, Rashid, S & Steege, R 2024, ‘Seven core competencies and conditions for equitable partnerships and power sharing in community-based participatory research’, BMJ Global Health, vol. 9, no. 11. https://doi.org/10.1136/bmjgh-2024-015497
Pascoe, KM, Petrescu-Prahova, M, Steinman, L, Bacci, J, Mahorter, S, Belza, B & Weiner, B 2021, ‘Exploring the impact of workforce turnover on the sustainability of evidence-based programs: A scoping review’, Implementation Research and Practice, vol. 2. https://doi.org/10.1177/26334895211034581
Pepler, D 2016, ‘Stepping sideways to move forward: Closing the science–practice gap’, Canadian Psychology/Psychologie canadienne, vol. 57, no.1, pp. 44–50. https://doi.org/10.1037/cap0000046
Pepler, DJ, Moore, T, Motz, M & Leslie, M 2002, Breaking the Cycle: The evaluation report (1995–2000), Toronto.
Pepler, DJ, Motz, M, Leslie, M, Jenkins, J, Espinet, SD & Reynolds, W 2014, The mother-child study: Evaluating treatment for substance-using women – A focus on relationships, Mothercraft Press.
Racine, N, Barriault, S, Motz, M, Leslie, M, Poole, N, Premji, S, Andrews, N, Penaloza, D & Pepler, D 2024, ‘A comparative effectiveness study of the Breaking the Cycle and Maxxine Wright intervention programs for substance-involved mothers and their children: Study protocol’, BMC Psychology, vol. 12, no. 1, p. 16. https://doi.org/10.1186/s40359-023-01484-w
Racine, N, Madigan, S, Cardinal, S, Hartwick, C, Leslie, M, Motz, M & Pepler, D 2022, ‘Community-based research: Perspectives of psychology researchers and community partners’, Canadian Psychology/Psychologie canadienne, vol. 63, no. 4, pp. 523–35. https://doi.org/10.1037/cap0000318
Reed, R 2015, ‘Program evaluation as community-engaged research: Challenges and solutions’, Gateways: International Journal of Community Research and Engagement, vol. 8, no. 1, pp. 118–38. https://doi.org/10.5130/ijcre.v8i1.4105
Robinson, E, Berg, P, McGowan, B & Tombs, B 2003, Maxxine Wright place project for high risk pregnant and early parenting women, https://atira.bc.ca/sites/default/files/assets/MaxxineWright.pdf
Rodríguez, GM, Garcia, D, Blizzard, A, Barroso, NE & Bagner, DM 2018, ‘Characterizing intervention strategies used in community-based mental health care for infants and their families’, Administration and Policy in Mental Health and Mental Health Services Research, vol. 45, no. 5, pp. 716–30. https://doi.org/10.1007/s10488-018-0855-0
Rutman, D, Hubberstey, C, Poole, N, Schmidt, RA & Van Bibber, M 2020, ‘Multi-service prevention programs for pregnant and parenting women with substance use and multiple vulnerabilities: Program structure and clients’ perspectives on wraparound programming’, BMC Pregnancy and Childbirth, vol. 20, no. 441. https://doi.org/10.1186/s12884-020-03109-1
Saleh, A, Saelens, B, Hayes, M, The Health Equity Community Advisor & Coker, TR 2022, ‘Community partnership guide for engaging with academic researchers’, Progress in Community Health Partnerships: Research, Education, and Action, vol. 16, no. 1, pp. 129–34. https://doi.org/10.1353/cpr.2022.0012
Skipper, Y & Pepler, DJ 2020, ‘Knowledge mobilization: Stepping into interdependent and relational space using co-creation’, Action Research, vol. 19, no. 3, pp. 588-605. https://doi.org/10.1177/1476750320960810
Springer, MV & Skolarus, LE 2019, ‘Community-based participatory research: Partnering with communities’, Stroke, vol. 50, no. 3. https://doi.org/10.1161/STROKEAHA.118.024241
Turnbull, AP, Friesen, BJ & Ramirez, C 1998, ‘Participatory action research as a model for conducting family research’, Journal of the Association for Persons with Severe Handicaps, vol. 23, no. 3, pp. 178–88. https://doi.org/10.2511/rpsd.23.3.178
Wallace, B, Pauly, B, Perkin, K & Ranfft, M 2015, ‘Shifting the evaluative gaze: Community-based program evaluation in the homeless sector’, Gateways: International Journal of Community Research and Engagement, vol. 8, no. 1, pp. 43–58. https://doi.org/10.5130/ijcre.v8i1.3936
Wallerstein, N 2021, ‘Engage for equity: Advancing the fields of community-based participatory research and community-engaged research in community psychology and the social sciences’, American Journal of Community Psychology, vol. 67, no. 3–4, pp. 251–55. https://doi.org/10.1002/ajcp.12530
Yoon, D, Snyder, SM & Yoon, S 2020, ‘Child maltreatment types and adolescent substance use: The role of deviant peer affiliation’, Child & Family Social Work, vol. 25, no. 2, pp. 355–63. https://doi.org/10.1111/cfs.12691