Gateways: International Journal of Community Research and Engagement
Vol. 16, No. 1
June 2023
PRACTICE-BASED ARTICLE
Oral Health Education for School Children and Capacity Building of Local Community Health Workers in Cleft Care: An Experience of Student-Led Community Service in a West Java Village
Erli Sarilita1,*, Adrina Kinindya Putri2, Arina Ghaida Faza3, Halimah Nisrina Mulyahati2, Jasmine Putri Anandita2, Nadia Elizabeth Annina3, Nur Aulya Hermalina4, Zulharistya Prima Sahda2
1 Department of Oral Biology, Faculty of Dentistry, Universitas Padjadjaran, West Java, Indonesia
2 Dental Medicine Study Program, Faculty of Dentistry, Universitas Padjadjaran, West Java, Indonesia
3 Pharmacy Study Program, Faculty of Pharmacy, Universitas Padjadjaran, West Java, Indonesia
4 Psychology Study Program, Faculty of Psychology, Universitas Padjadjaran, West Java, Indonesia
Corresponding author: Erli Sarilita, Faculty of Dentistry, Universitas Padjadjaran, West Java, Indonesia, erli.sarilita@unpad.ac.id
DOI: https://doi.org/10.5130/ijcre.v16i1.8594
Article history: Received 29/03/2023; Revised 15/06/2023; Accepted 26/07/2023; Published 08/2023
Abstract
This article presents a program that seeks to establish partnerships between universities and rural villages in West Java provinces, with a focus on health-related activities. The program involves undergraduate students participating in field studies in the community through three activities: educating school children about oral health, providing capacity building for community health workers in managing infants with cleft, and assisting community health workers at Integrated Service Post (Posyandu). The program was developed by scholars at Universitas Padjadjaran and West Bandung Regency of West Java Province to contribute to the development of neighbouring regions. The program has had two significant impacts. First, the undergraduate students are directly involved in the community and can reflect on what they have learned in the context of the community, while also earning credits towards their transcripts. Second, the program has had a positive impact on healthcare by educating various community groups on topics ranging from oral health to early management of infants with orofacial clefts. This program serves as an example of how academic study and community service can be successfully combined to produce positive outcomes for both the students and the community.
Keywords
Community-University Partnerships; Indonesia; Oral Health Education; Capacity Building; Cleft Lip and Palate; Community Health Workers
Introduction
Higher education has a crucial role to play in enhancing both society and academia. It is thus important for academics, as significant recipients of higher education, to participate in community involvement (Kearney et al. 2013). One of the important ways in which the academics at Universitas Padjadjaran are evaluated is through their involvement in community-engagement activities (Sarilita et al. 2022). The community involvement program at Universitas Padjadjaran can be implemented in one of two ways: integrated in the curriculum as a learning activity for students, whereby they can earn academic credits under the guidance of faculty members, or as an independent project led by faculty members themselves. The undergraduate degree curriculum at Universitas Padjadjaran incorporates a Community Service course, which is mandatory to completing the degree. This course requires students to work in a group of 15 under the guidance of one lecturer, and to stay in a village in a rural area of West Java province for two months to try to address community health issues. Approximately 7000 undergraduate students in their second to third year are deployed annually in two batches. Prior to their deployment, partnerships are established between Universitas Padjadjaran and the local government. The work that the students do in the village is supervised by the academic staff of Universitas Padjadjaran, and the scope of the work that the students do varies, depending on the supervisor’s expertise and research interests, which may range from health, science, engineering and humanities to agriculture, in line with the diverse study program at Universitas Padjadjaran. In addition, the supervisor suggests the preferred location, which is usually based on whether the intended area has been covered with the community service in the topic.
According to the World Health Organization (2023), about 3.5 billion people worldwide suffer from oral diseases, with three out of every four of these individuals residing in middle-income nations. Five hundred and fourteen million children worldwide suffer from primary tooth decay, while two billion adults are thought to have permanent tooth decay. Most oral health disorders can be treated when they are in their early stages. Dental caries (tooth decay), periodontal disorders, tooth loss and oral malignancies account for most occurrences. Orofacial clefts, noma (a severe gangrenous disease that begins in the mouth and primarily affects youngsters) and oro-dental trauma are further oral disorders of public health significance (WHO, 2023).
This article reflects our community-university partnerships in student-led activity at Universitas Padjadjaran in a West Java village. The activity was conducted between January and February 2023 and took the form of oral health education for elementary school pupils and cleft care capacity building for community health workers. This article is divided into five sections. The first covers the general description of the location where the program was performed, including the overall geographical and logistical details, followed by the activities covered in this university-community partnership which are divided into two sections that correspond to the different themes. The second section focuses on oral health education for elementary school children, including the background to the activities. The third section concentrates on the building of capacity for community health workers in managing babies born with cleft lip and or palate and the rationale for creating the program. The fourth section describes the students’ program of giving helping hands to community health workers through monthly activities and monitoring mother and child health (Posyandu). The last section includes a reflective analysis based on the students’ voice and the challenges met, along with the proposed pathway to address them.
General geographical and logistical details
Jambudipa village is located in Cisarua district, West Bandung regency West Java province in Indonesia and covers an area of 1.45 square kilometres. The number of inhabitants in the village is 14,610. The density level at this village is 10.076 residents per square kilometre, which is considered high compared to other areas in the province. The main economic production/revenue of Jambudipa village is produced through agriculture and dairy farming.
The regular practice of community service by the Universitas Padjadjaran involves a registration process for the academics, along with the proposed programs and locations, which is listed in the academic system. The students who are planning to take this community service module then have to select the desired supervisor, program and location by inputting four options from among the available programs. The academics then approve the chosen applicants on a first come, first serve basis to fulfil the quota, which usually is 15 students. Hence, the interdisciplinary collaboration background in community service at Universitas Padjadjaran is aimed at, and contingent upon, the composition of the final student group. In this case, the community service team from Universitas Padjadjaran, which serves Jambudipa village, consisted of one academic with a dentistry background as the project supervisor and 15 undergraduate students in their fifth semester: four dental students, three medical students, three pharmacy students, four psychology students and one communication science student.
This community service course, which contributes towards the credit earning of the academic transcripts, receives funding from the Directorate of Research and Community Service at Universitas Padjadjaran in each semester. As mentioned above, there are approximately 7000 students involved each year, in two cohorts. The number of students varies, depending on how many students are receiving credits for community service in each semester, but each cohort can involve 200–300 community service programs led by 10 to 17 students per program. Each community service program receives funding between IDR 5 million (+/- USD 334) and IDR 10 million (+/- USD 668) depending on the distance between the target location and the Universitas Padjadjaran. The funds are allocated to coordination and implementation of community service initiatives.
Oral health education for school children
Oral diseases have emerged as a global public health concern that demands attention (Peres et al. 2019). Several behavioural and social characteristics, including dietary habits, oral health awareness and practices, and accessibility to oral health services, are significant determinants of oral health. Educational and behavioural interventions aimed at promoting good oral hygiene practices and controlling the impact of social and mental factors on dental health behaviour are necessary to mitigate oral health problems and promote oral health (Martino 2011). According to the WHO Global Oral Health Status Report (2022), approximately 514 million children are affected by primary teeth caries. In this regard, oral health education programs play a pivotal role in preventing oral diseases, mitigating oral health problems and promoting oral health, particularly in rural areas. At the 74th World Health Assembly, the World Health Assembly endorsed a Resolution on oral health in 2021. The Resolution advocates for a transition from a conventional focus on treatment to a preventive approach, which involves promoting oral health in family, school and workplace settings (WHO 2023).
Based on the results of Indonesia Basic Health Research (Riskesdas) in 2018, approximately 57.6 per cent of the Indonesian population is experiencing dental and oral health problems. From that research data, only 10.2 per cent of the population has received dental health services. It was also stated that Indonesia still has a very high prevalence rate of cavities in early childhood, which is about 93 per cent, which indicates that only about 7 per cent of children are free from cavities. Only 2.8 per cent of the Indonesian population practises proper tooth brushing (Riskesdas, 2018). This fact drove the team to perform oral health education in Jambudipa village.
Collaborative approach to implementing the oral health program
The team initially conducted a survey at the local government office to gain information on elementary schools in Jambudipa village. Four out of fifteen students were dental students and thus were responsible for creating the oral health education content. A total of seven elementary schools, five in the Jambudipa village and two from the neighbouring village (Tugumukti), were chosen to be covered by the program due to the local government’s request not to leave any school behind as they strongly supported the program (SDN Jambudipa 1, SDN Jambudipa 2, SDN Harapan Mekar, SDN Gandrung Endah, SDN Barukai, SDN Tugumukti and SDN Tugurahayu).
Due to time constraints, it was necessary to select which level students would be addressed first and the team chose students in Grades 3 and 4. However, the target students were then changed to Grades 3 and 6 after discussion with the local government so that there would be representation at the lower level (Grade 3) and at the higher level (Grade 6). The team then met with the principal of each of the seven schools that were targeted after engaging with relevant stakeholders.
Each school took a day in execution. The 15 students were divided into three classes per school and the oral health education was conducted using flip charts, children’s songs and storytelling. Before starting the storytelling session, school children were given a test on the material to be delivered, followed by a post-test using the same questions and an evaluation of their reactions. The storytelling provided material about dental and oral health methods to make it easier to understand and create a more interactive atmosphere, as well as short quizzes, games and assessments (Figure 1a). The activity was concluded with step-by-step practice on how to brush teeth properly. Each session lasted for two hours. In total, after seven days of training, 867 school children received oral health education. These learning sessions attracted the attention of the dental related corporations, which gave their support by providing the toothpaste and toothbrushes that were given to the students.

Figure 1. a. Oral health education session at Jambudipa I elementary school; b. Focused group discussion session on dealing with babies born with cleft; c. Dental consultation at the Posyandu in Jambudipa village.
Evaluation of the oral health program
Achievement of activities was measured at two levels. The first level was carried out through reaction evaluation, an assessment that measures the experience and satisfaction of target participants while participating in educational activities. The second level was carried out through learning evaluation via a pre-test and post-test to determine the increase in students’ understanding before and after dental and oral health education.
Based on the results of the evaluation of reactions, it can be concluded that all students participating in education generally enjoyed participating in educational activities and found these activities interesting. In addition, participants also felt they could understand the material presented and were motivated to join because they wanted to keep their teeth and mouth healthy. The percentage of reaction evaluation results can be seen in Table 1.
The results of the learning evaluation were processed using the Wilcoxon Signed Rank Test because each item’s type of data is ordinal. The analysis of statistical tests was carried out in two stages. The first was an analysis of the success of learning objectives determined from five pre-test and post-test questions, with indicators of achievement for each item being 71%, or 5 out of 7 schools attaining significant changes in each learning objective. The results of the analysis of each item are listed in Table 2. The second was an analysis of learning success as seen from the overall score for the pre-test and post-test at each school. A Wilcoxon Signed Rank Test showed that oral health education intervention elicits statistically significant changes in item 1 and item 4 test scores and total test scores (p<0.001) (Table 3).
| Item 1 | LO: Students can name the types of teeth. There was a significant change in the results of the pre-test and post-test in 7 out of 7 schools so that the learning objectives that had been prepared were achieved by 100% and exceeded the achievement indicator, which was 71%. |
| Item 2 | LO: Students can name foods that are harmful and good for teeth. There were significant changes in the results of the pre-test and post-test in 4 out of 7 schools, so the learning objectives that had been prepared were only achieved by 43%, less than the achievement indicator, namely 71%. |
| Item 3 | LO: Students can name an excellent time to brush their teeth. There were changes in the results of the pre-test and post-test in 4 out of 7 schools, so it can be said that the learning objectives that had been prepared were only achieved by 57%, less than the achievement indicator of 71%. |
| Item 4 | LO: Students can name a reasonable amount of time to brush their teeth. There was a significant change in the results of the pre-test and post-test in 6 out of 7 schools, so it can be said that the learning objectives that had been prepared were achieved by 86% and exceeded the achievement indicator, namely 71%. |
| Item 5 | LO: Students can distinguish between good and bad teeth (toothache). The results of the pre-test and post-test remained the same n=7 out of 7 schools because students already understood the learning objective before the material was delivered. This can be seen from the data answers of each student. |
| Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Total | |
|---|---|---|---|---|---|---|
| Z | -10.997b | -3.976b | -4.315b | -14.500b | -.566b | -14.943b |
| Asymp. Sig. (2-tailed) | 0.000 | 0.000 | 0.000 | 0.000 | 0.572 | 0.000 |
a. Wilcoxon Signed Ranks Test
b. Based on negative ranks
The results can be seen in Figure 2 and Table 4. Based on the total scores of each school for the pre-test and post-test, it was found that only one school, namely Tugurahayu, had insignificant results (p > .05) with t(49) = 1.420, p = .162. This shows that the material given regarding oral health has yet to significantly impact the understanding of students at SDN Tugurahayu. Meanwhile, the statistical test results for the other six schools were significant, as shown in Table 4, so the material provided increased students’ understanding of dental and oral health.
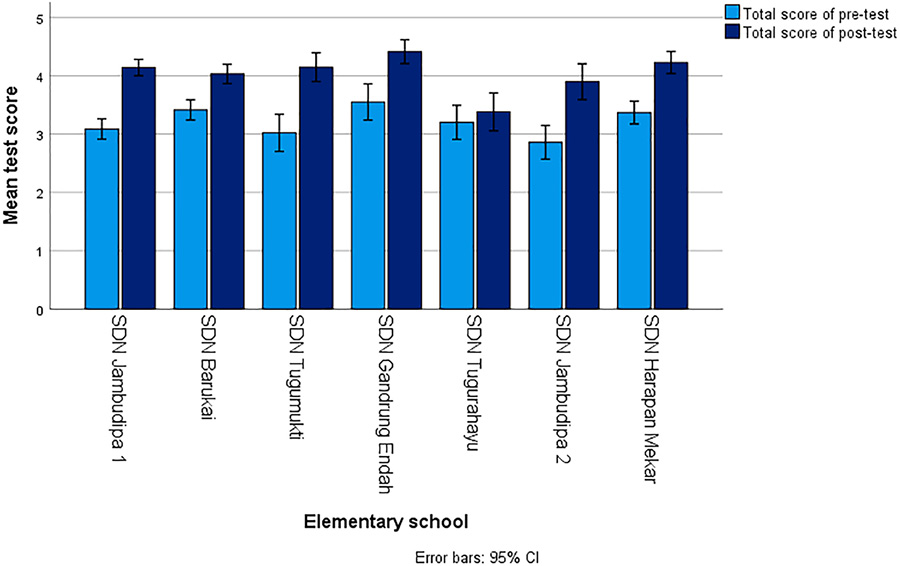
Figure 2. Wilcoxon bar chart comparing total score of pre-test and post-test in different elementary schools.
Capacity building for community health workers in early management of infants with cleft
Continuing the work in the field of community service in healthcare, the subsequent section focuses on enhancing the capabilities of local health workers in cleft care through capacity building initiatives. Cleft lip and palate (orofacial cleft) are congenital conditions that affect the orofacial area. The types are cleft lip, cleft palate, or both. A cleft lip occurs when the tissue that forms the lip fails to fuse completely before birth (between the fourth and seventh weeks of pregnancy). Cleft lip can be on one or both sides of the lip or in the middle of the lip. Cleft palate happens when the tissue that forms the roof of the mouth fails to fuse completely before birth (between the sixth and ninth weeks of pregnancy) (Mossey et al. 2009).
Having a cleft lip and/or palate can affect the quality of life of these people, including their self-esteem and social relationships (Gulsen 2020). Thus, we chose to make an educational program on cleft lip and palate for community health workers as the main topic of our community service activities to increase their knowledge of the treatment and management of these conditions. We undertook the program in the form of presentations on the topic of ‘Introduction to Cleft Lip and Palate’, delivered by students of the Faculty of Dentistry, and ‘Quality of Life for Families and Patients with Cleft Lip and Palate’, delivered by students of the Faculty of Psychology.
This activity began with a meeting with the chief of Cisarua Health Center and the head of Jambudipa Village to explain the plans regarding the counselling activities that we would undertake and to hold joint discussions to set targets and timelines for the program’s implementation. Considering the significant number of community health workers in Cisarua Sub-District, totalling more than 500, we made the decision to focus our efforts on a target group of 51 individuals. This group would comprise three community health workers from each community unit. We then scheduled the program to commence after completion of our initial activity, which involved providing dental and oral health counselling to elementary school students, concluding at the end of January.
After the meeting with the local stakeholders, we held a discussion to determine the best way to carry out the activity. We came up with the idea of providing interactive teaching in the form of two lectures on topics such as cleft lip and palate in general and the quality of life for families and people with cleft lip and palate. In both lectures, there was a focus group discussion (FGD), in which participants were divided into four groups and assisted by two facilitators as they discussed procedures for dealing with babies born with cleft lip and palate. At the end of the activity, participants were asked to fill out a feedback form, which could be exchanged for lunch. The preparation process was followed by a discussion on the technical implementation of the event, specifically about task division, preparation of the materials and equipment, and deciding on the date and location of the activity. This event took place in the Jambudipa Village Office Hall on Monday, 30 January 2023 at 10 a.m.
The event began with the MC’s opening remarks and words from several key participants, such as the leader of the group (AKP), the secretary of Jambudipa Village and the Cisarua District Midwife. Following this was a presentation on Cleft Lip and Palate (CBL) by the dental student team, and then a Focus Group Discussion (FGD) on dealing with babies born with CBL (Figure 1b). During the FGD activities, participants were asked to discuss and arrange the order of treatment when a baby was born with CBL on a board. The main facilitator then provided an explanation of how to handle CBL and match it with the participants’ answers. After the FGD was finished, the psychology team presented the most recent material on the topic of quality of life of families and CBL patients. The activity concluded with the completion of the feedback form, the awarding of certificates, and a photo session of all participants and the committee. Out of the 51 community health workers that were initially targeted by the group members, 47 attended the program, which consisted of 39 community health workers from several community units, 7 members of the Family Welfare Programs’ working groups, and 1 midwife from the Cisarua sub-district.
An analysis of the feedback form (Table 5), which was completed by 36 participants, showed that all participants agreed or strongly agreed that the material provided was useful and that they understood it. The participants also said that the material presented was interesting. However, around 8.4 percent of the participants thought that the timing and duration of the program inadequate.
| Responses | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| I felt that the material presented was useful | 0 | 0 | 27.8 | 72.2 |
| I understood the material that was presented | 0 | 0 | 72.2 | 27.8 |
| I found the way the material was presented was interesting | 0 | 0 | 66.7 | 33.3 |
| I thought that the timing of the event was good | 0 | 2.8 | 83.3 | 13.9 |
| I felt that the duration of the event was sufficient | 0 | 5.6 | 80.6 | 13.9 |
*1 Strongly disagree; *2 Disagree; 3* Agree; 4* Strongly agree
The method used in this capacity-building program was a series of lectures with an interactive group discussion in between. The first lecture was given by the dental students’ team on the clinical aspects of cleft lip and palate to familiarise the audience with the topic. In this part of the event, the audience mainly learned about the causes of clefts and their prevention.
The next segment was an interactive group discussion to inform community health workers how to manage babies born with cleft. The audience was asked to arrange a series of cutout cards in their correct order, which would be checked by the main facilitator at the end of the session. All of the audience members actively participated in the activity and the group discussion.
The final segment was a lecture on the quality of life of cleft patients and their surroundings, which was presented by the student psychology team. This segment was included to show the community health workers what things could be an obstacle for cleft patients and their families in their daily lives within the community, in the hope that all of the community health workers would be able to empathise with them.
Overall, all of the programs that were undertaken by the group members received great responses, both from the local community and other stakeholders. The results from the feedback form also indicated that the majority of participants understood and felt that the activities undertaken were useful. In future, we might need to provide similar or related activities in order to maintain community health workers’ knowledge regarding cleft lip and palate, and its treatment.
Assisting community health workers at Integrated Service Post
The Indonesian health system starts at the smallest unit, which is called the Integrated Service Post (Posyandu). Posyandu is a form of Community Based Health Effort (Upaya Kesehatan Bersumberdaya Masyarakat, UKBM) carried out by, from and with the community, to empower and provide convenience to the community in obtaining health services for mothers, infants and toddlers. Posyandu’s main activities include community monitoring and education on the health of mother and child, family planning, immunization, nutrition, and the prevention and control of diarrhea (Centre for Health Promotion, Ministry of Health 2012). Posyandu is run by local community health workers. Community health workers in Indonesia, also known as Kader Kesehatan, play a vital role in providing primary healthcare services and promoting health awareness within their communities. Community health workers typically undergo training programs conducted by the Ministry of Health or local health authorities. These programs equip them with basic healthcare knowledge and skills to deliver essential health services at the community level. The training covers areas such as maternal and child health, family planning, immunisations, basic healthcare practices, health education and disease prevention. Community health workers in Indonesia are often considered voluntary or semi-voluntary workers who provide their services on a community-based or part-time basis. The compensation received by community health workers can vary, depending on the region and the local healthcare system.
The introduction of the community service program resulted from an audience with the Head of Jambudipa Village, where the activity plan was explained, along with a proposal for a checkpoint for measuring blood pressure and a dental consultation service as the integrated services post-activities (Figure 3). Following the audience, the team was directed to further discuss this with the head of Jambudipa Village as well as the chief of local health workers. Based on the outcomes of the discussion, it was discovered that Posyandu activities were carried out in each community unit (RW), with a total of 18 Posyandu in Jambudipa Village, following the number of RWs, which run once a month. Due to the time constraint, the community service program was scheduled to assist 3 out of 18 Posyandu activities. The general health and dental health checkpoints are implemented by adding two check-in desks to the Posyandu flow as follows:
1. Parents collect data at the administration post.
2. Toddlers’ weight and height, as well as head circumference and arm circumference, are measured.
3. At the dental checkpoint, toddlers are instructed to have a dental examination.
4. At the public health post, parents check their blood pressure and provide data on complaints and medical history.
Each of the sessions lasts for four hours. Attendees at Posyandu range from 40–44 mothers, 1–5 expectant mothers and 30–36 toddlers.
Pedagogical aspect and reflective analysis from student perspective
The community service module in higher education yields diverse and valuable learning outcomes. It cultivates civic engagement, as students become actively involved in addressing social issues within their communities. In this community service module, various learning methods are employed to enhance student engagement and facilitate active learning. These methods include experiential learning, where students not only directly participate in community activities, but also live in the community, reflecting on their experiences and drawing lessons from them (Table 6). Collaborative learning is encouraged through working on this community service project, allowing students to work together, share ideas, and learn from one another. Service-learning combines academic instruction with community service, providing opportunities for students to apply their knowledge and skills to real-life situations. Reflection activities, such as group discussions, are incorporated to encourage critical thinking and deeper understanding. These diverse learning methods create a dynamic and enriching educational experience for students participating in the community service module.
The process of appointing the group leader and organising division for this student-led community service project was carried out without any interference from the supervisor. The selection of the group leader was likely based on various factors, such as leadership qualities, relevant knowledge and skills and a demonstrated commitment to the project’s objectives.
The students encountered some difficulties when engaging with the communities, the first being their disengagement during oral health education. This could be attributed to a lack of pedagogical skills in engaging elementary school-age children. Moreover, some citizens living in these particular rural areas still use dialects rather than the national language, which poses a challenge for communication. The request by the local government that the student working group cover all targeted units in the area also remained unfulfilled due to limited working time and human resources. To further complicate the problem, certain elementary schools were difficult to reach in terms of transportation access and distance.
Program outcomes
The current capacity-building program can only reach an audience in one village, namely Jambudipa Village, where the audience consisted of 39 community health workers from several community units, 7 members of the Family Welfare Programs’ working groups and 1 midwife from the Cisarua sub-district. Although the current program is able to reach only a small audience, the event can be held effectively, as the audience focuses more on listening to the presenters because they are in the same room, and presenters can monitor and pay attention to the audience. In addition, offline activities allow the audience to socialise more easily with one another. Lectures, Focus Group Discussions (FGD) and Question and Answer sessions can also be more interactive if offline rather than online. This program succeeded in contributing to increased understanding of the incidence of cleft lip and palate and was well received by the participants according to the results of the reaction survey. Based on the results of the local community health workers’ feedback, there were several matters from the authors’ perspective that needed to be improved, such as the short duration of the program and the explanation of some of the medical terms that had been difficult for the participants to understand.
In addition to cleft lip and palate educational activities, we held dental and oral health education activities for children aged 6–12 years, or elementary school age. This program was conducted using a storytelling method, which helps to develop creativity and imagination, expand ways of thinking, and offer different life experiences to children (Cohrssen et al. 2016). At the end of the event, we held a quiz, with prizes for the children.
The educational programs discussed in this article have succeeded in contributing to development of knowledge and increasing interest in the oral and dental health of elementary school-age children in Jambudipa Village. This can be seen in the achievement of the learning objectives and the enthusiasm of the pupils participating in this program. Due to limited time and human resources, the program was only conducted in a few schools in the Cisarua sub-district and in certain classes in every school. It would have been beneficial if more schools had been involved in the program. Our plan is to regularly hold similar oral health activities for elementary school students at least once a year. This needs to be done, so that oral health becomes a habit for participants and is not just attended to during their education. We also consider that future programs should be carried out in different locations in order to spread the message of oral health evenly.
An aspect that was overlooked was the inclusion of cleft lip/palate education for school children with those conditions, to mitigate the stigma they face. These children are vulnerable to bullying and other social challenges within the school environment. Conducting such an intervention in the future would be highly valuable and impactful in raising awareness, promoting acceptance, and fostering a supportive atmosphere for children with cleft.
Next steps
The sustainability of the community-university partnerships at Universitas Padjadjaran is ingrained in and integrated with academic key performance indicators. Each batch of community service courses for undergraduate students has different themes, depending on the partner that reaches out to us, for example, the ministry, NGO or industry.
In conclusion, community-university partnerships are essential to conducting successful community service programs and ensuring their sustainability. These partnerships bring together the resources, expertise and knowledge of both the community and the university to tackle social issues and improve the quality of life for individuals and communities. Through collaborative efforts, community-university partnerships create meaningful, long-lasting changes that benefit everyone involved. Furthermore, partnerships foster a sense of community ownership and engagement, ensuring the continued success and sustainability of the programs beyond their initial implementation. This practice-based article is intended to serve as a lesson for similar programs in the future, especially in Indonesia and/or neighbouring regions, to emphasise the importance of fostering and supporting community-university partnerships, so as to build stronger, more resilient communities that thrive and flourish.
References
Badan Pusat Statistik Kabupaten Bandung Barat 2021, Badan Pusat Statistik Provinsi Jawa Barat. https://bandungbaratkab.bps.go.id/indicator/153/88/1/tinggi-wilayah-dan-jarak-ke-ibukota-kabupaten-menurut-kecamatan.html
CDC, Basics of oral health. https://www.cdc.gov/oralhealth/basics/index.html
CDC, Cleft Lip / Cleft Palate. https://www.cdc.gov/ncbddd/birthdefects/cleftlip.html
Centre for Health Promotion, Ministry of Health, Buku saku posyandu (pocket book of the Integrated Healthcare Center) 2012. https://promkes.kemkes.go.id/fact-program-prom---posyandu
Cohrssen, C, Niklas, F & Tayler, C 2015, ‘Is that what we do? Using a conversation analytic approach to highlight the contribution of dialogic reading strategies to educator-child interactions during storybook reading in two early childhood settings; Journal of Early Childhood Literacy, vol. 16, pp. 361–82. https://doi.org/10.1177/1468798415592008
Disdukcapil Kabupaten Bandung Barat 2019, ‘Geographic Information System (GIS) Kab. Bandung Barat Kecamatan Cisarua dan 8 desa.’ https://disdukcapil.bandungbaratkab.go.id/Home/gis/cisarua
Gulsen, A, ‘Current treatment of cleft lip and palate’. https://doi.org/10.5772/intechopen.77803
Kearney, J, Wood, L & Zuber-Skerritt, O 2013, ‘Community-university partnerships: Using participatory action learning and action research (PALAR)’, Gateways: International Journal of Community Research and Engagement, vol. 6, pp. 113–30. https://doi.org/10.5130/ijcre.v6i1.3105
Martino, S 2011, ‘Oral health behavioral and social intervention research: Concepts and methods’, Journal of Public Health Dentistry, vol. 71, suppl. 01, pp. 2–6. https://doi.org/10.1111/j.1752-7325.2011.00217.x
Mossey, P, Little, J, Munger, R, Dixon, M & Shaw, W 2009, ‘Cleft lip and palate’, The Lancet, vol. 21, no. 374 (9703), pp. 1773–85. https://doi.org/10.1016/S0140-6736(09)60695-4
Peres, M, Macpherson, L, Weyant, R, Daly, B, Venturelli, R, Mathur, M, Listl, S, Celeste, R, Guarnizo-Herreno, C, Kearns, C, Benzian, H, Allison, P & Watt, R 2019, ‘Oral diseases: A global public health challenge’, The Lancet, vol. 2019, no. 394, pp. 249–60. https://doi.org/10.1016/S0140-6736(19)31146-8
Riskesdas, Potret Sehat Indonesia dari Riskesdas 2018. https://www.kemkes.go.id/article/print/18110200003/potret-sehat-indonesia-dari-riskesdas-2018.html (accessed 2 March 2023).
Sarilita, E, Nugraha, H, Murniati, N & Soames, R 2022, ‘Online capacity building in anatomy knowledge for high school biology teachers: Community-university partnerships in Indonesia during the Covid-19 pandemic’, Gateways: International Journal of Community Research and Engagement, vol. 2022, no. 1, pp. 1–9. https://doi.org/10.5130/ijcre.v15i1.8043
WHO 2022, ‘Global oral health status report: Towards universal health coverage for oral health by 2030’, World Health Organization. https://www.who.int/publications/i/item/9789240061484
World Health Organization 2023, Oral health. https://www.who.int/news-room/fact-sheets/detail/oral-health