Vol. 16, No. 1
October 2023
Snapshot article
Stroke Community Rehabilitation Centre (SCORE): A Community Transformation Program
Beh Wen Fen1 and Lydia Abdul Latif2
1 Senior Lecturer, Department of Music, University Malaya, Kuala Lumpur, Malaysia
2 Professor, Department of Rehabilitation Medicine, University Malaya, Kuala Lumpur, Malaysia; Chief Medical Officer, Department of Rehabilitation Medicine, ReGen Rehab Hospital, Selangor, Malaysia
Corresponding author: Beh Wen Fen, Senior Lecturer, Department of Music, University Malaya, Kuala Lumpur, Malaysia, beh.wenfen@um.edu.my
DOI: https://doi.org/10.5130/ijcre.v16i1.8583
Article history: Received 22/03/2023; Revised 05/05/2023; Accepted 20/09/2023; Published 10/2023
Abstract
Stroke is the second most prevalent disease in Malaysia, so promoting awareness of stroke is essential as it is preventable and treatable if action is prompt. Long-term rehabilitation at the community level is also crucial to reducing congestion in acute care hospitals. Hence, establishing an evidence-based community rehabilitation centre would help educate the community and support the welfare of stroke survivors.
This article discusses a community-engagement initiative launched by experts from University Malaya Rehabilitation Medicine in partnership with Pusat Pemulihan Kesihatan (PERKIM), a religious and social welfare organisation in Malaysia, to transform an existing non-functional community centre run by PERKIM into the Stroke Community Rehabilitation Centre (SCORE). This was achieved through the provision of expert input into how to improve service provision, knowledge transfer to the community, and implementation of more thematic and creative components to the model of care currently offered. Importantly, under this new model, stroke survivors and the wider community would be considered learners and active participants in their own care, not mere passive recipients of charity.
Since its inception in 2016, the number of patients has almost doubled, increasing to over 100. Thus, the Stroke Community Rehabilitation Centre benefits the stroke community by providing resources and education to facilitate recovery at a reduced cost to hospital-based care. With its adherence to the recommended features of the community-based rehabilitation model, as outlined by WHO, the success of SCORE is an exemplary model for future stroke community rehabilitation centres in Malaysia.
Keywords
Community Engagement; Stroke Community Rehabilitation Centre (SCORE); Stroke; Stroke Survivors; University Malaya Rehabilitation Medicine
Introduction
Stroke is a leading cause of disability in adults. In Malaysia, there were 47,911 incidents, 19,928 deaths, 443,995 prevalent cases, and 512,726 disability-adjusted life years lost due to stroke in 2019 (Tan & Venketasubramanian 2022). As the second most common disease in Malaysia – after cardiovascular diseases – it is important to promote awareness of this issue as stroke is preventable and treatable if immediate action is taken. Following a stroke, a person’s condition can deteriorate rapidly, reducing their quality of life (GBD 2015). As stroke is a life-long condition, rehabilitation is the cornerstone of stroke treatment. Hence, it is important to provide long-term rehabilitation at the community level to reduce congestion in acute care hospitals.
In this article we discuss a collaborative project aimed at transforming an existing but ailing centre into a sustainable and evidence-based community rehabilitation centre, as well as an effective model for promoting the welfare of stroke survivors and providing lifelong learning for the stroke community (survivors and their families and carers). Thus, it is hoped that the Stroke Community Rehabilitation Centre (SCORE) will benefit the stroke community by granting them access to the resources they need in their journey towards recovery.
To successfully establish SCORE, it was crucial that the concept focus on the community. In bringing in university-based experts to contribute evidence-based practice and empirical evidence, consideration was given to the practical aspects of providing care for stroke patients in a real-world setting. This included appropriate training for the staff at the centre, as well as a focus on educating the community at large to give patients agency over their rehabilitation journey. Raising awareness of stroke prevention and treatment was also important for SCORE to fulfil its purpose.
The implementation of a dedicated rehabilitation centre within the community will have a major impact as it can help raise awareness of stroke (Clarke & Forster 2015). Based on research conducted by researchers at Universiti Malaya (UM), it was found that the medical expenditure of stroke survivors was high (Akhavan et al. 2015). The SCORE project leader and team members also conducted a survey to assess the availability of stroke rehabilitation services within the Klang Valley region. People in the community reported that there was limited access to these services, especially on the east coast of Malaysia. The Klang Valley constitutes an urban cluster in Malaysia, its focal point being located within the federal territories of Kuala Lumpur and Putrajaya. It also encompasses the surrounding cities and municipalities situated in the state of Selangor. Another study identified a higher risk of cognitive impairment and fatigue in stroke survivors (Rutkowski, Sabri & Yang 2021). Furthermore, based on the findings of our research, chronic stroke survivors were more susceptible to depression and spasticity, which negatively affected their recovery (Mohd Zulkifly et al. 2016). Another study conducted by UM researchers observed that the rate of return to work post-stroke was 49.5 percent (Jee & Abdul Latif 2017). Thus, as there is a high occurrence of stroke in Malaysia (Department of Statistics Malaysia n.d.), it is important to educate the public on the risks of stroke. Furthermore, fostering a bond between the public and academia would promote an understanding by the community of how research efforts pertaining to stroke benefit society.
Transforming an ‘ailing’ model of health care into community-based rehabilitation: Approach and implementation
In implementing this project, SCORE incorporated approaches introduced in the Quadruple Helix Model (Figure 1), where cooperation and participation between the government, universities, industries and the community continue to be enhanced and strengthened (Caravannis & Campbell 2009). At SCORE, a team of academics are involved in the development of educational programs curated to meet the needs of the stroke community. This is considered integral to the rehabilitation process as active participation from the community will provide ongoing insights into improving the current program. The Islamic Welfare Society of Malaysia (PERKIM) is an organisation that supports various welfare activities involving preaching, education and general health. It is also involved in the stroke community collaboration with the Universiti Malaya Medical Center (UMMC). PERKIM was central to the project through its allocation of resources to community-based rehabilitation programs. The National Blue Ocean Strategy (NBOS), a government-mandated national development strategy, was also key to these efforts as it maximises community participation through strategic allocation of the involved parties, allowing the stroke community to effectively implement professional advice. NBOS was formulated and executed through the NBOS Summit, a unique and dynamic national strategy platform, which brings together ministries, agencies, all levels of government and the private sector on a voluntary basis to develop initiatives that are high impact, low cost and rapidly executed. In utilising the Quadruple Helix Model, it was hoped that SCORE would positively impact the stroke community, including the patients’ families and caregivers, which it did! A once non-functional community centre was transformed into SCORE, a sustainable community-based rehabilitation (CBR) centre in a strategic location aimed at helping stroke survivors in underprivileged communities.
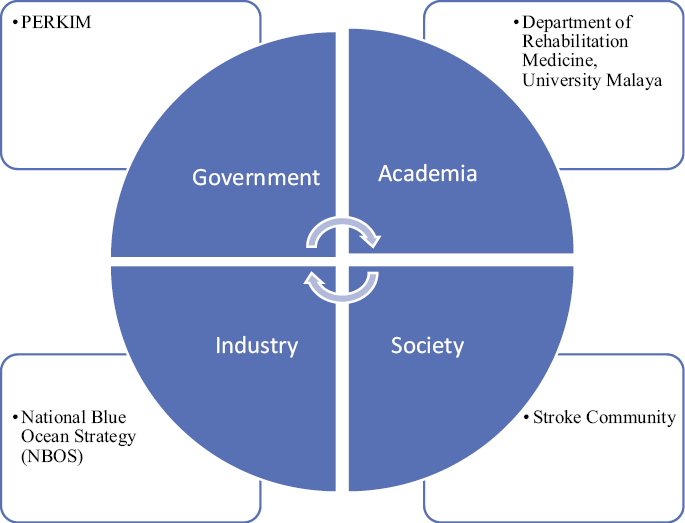
Figure 1. Quadruple Helix Model
The project had four main objectives:
1. To transfer and scale up an ‘ailing’ community centre through Knowledge Transfer from academia to community.
2. To provide expert input to improve service provision.
3. To improve the current model of health care with more thematic and creative components.
4. To ensure long-term sustainability by improving the program through the provision of continued and ongoing care, as well as active patient involvement and insights.
The community-engagement initiative was launched in 2016 by a team of experts from the Department of Rehabilitation Medicine, UM, in partnership with PERKIM. The team includes a medical rehabilitation doctor, an occupational therapist, a physiotherapist, a speech therapist, a nurse and a research assistant. The project is supported by a UMCares grant as well as collaboration with the National Blue Ocean Strategy (NBOS).
Central to the project was the belief that a charity model would not be a feasible foundation for sustainable CBR, so the concept adopted by the CBR centre was ‘for community, by community’. Through our research, in collaboration with industry experts from non-governmental organisations focused on improving the wellbeing of the underserved communities, we identified that community rehabilitation centres in the Klang Valley area, as well as other regions of Malaysia (1) were not run by medical personnel; (2) did not receive any input from medical experts; (3) were run on a charity model; (4) were poorly maintained, and (5) lacked facilities that are essential to the rehabilitation process.
The previous centre lacked trained manpower and the facilities were not conducive to patients’ rehabilitation. Prior to the intervention, the centre was not equipped to effectively provide rehabilitation to stroke patients. As seen in Figure 2, treatment was not provided by a physiotherapist and the equipment available was dated and inadequate. Although patients frequented the centre to receive treatment, they were not receiving optimal care due to there being limited facilities and staff.

Figure 2. Prior to the launch of SCORE, the rehabilitation centre was in a dilapidated state and the equipment was dysfunctional. There was also a lack of trained staff to provide care.

Figure 3. After the launch of SCORE, the rehabilitation centre was fitted with new equipment and new staff were trained, allowing effective provision of rehabilitative care to more stroke patients.
This project emphasised the need for a cost-effective rehabilitation centre that could be established within a short time frame. Experts from the university were brought in to assist in transforming the centre. This was done through collaborative workshops and interactive seminars, in which rehabilitation physicians and therapists shared their expertise in evidence-based practice, as well as the latest advances in stroke care, with the centre’s multidisciplinary team. With the funding available, the centre was able to be renovated and fitted out with improved equipment that would assist patients in their rehabilitation process. New staff, including a physiotherapist, an occupational therapist and a speech therapist, were recruited to provide appropriate care for the patients.
Not only that, instead of establishing a new rehabilitation centre, it was decided to renovate the existing centre. SCORE was set up with a budget of RM 75,000, much less than the cost of building a new rehabilitation centre (RM 250,000). It took two months to renovate the existing centre, compared to the 18 months it would have taken to build a new centre. Fostering long-term collaboration via the signing of the Memorandum of Agreement (MoA) between the university and the community also minimised the cost and ensured the sustainability of SCORE.
Along with its re-launch as SCORE, the centre was transformed through expert planning to accommodate more patients, upgrade facilities, recruit new staff and provide care at a reduced cost. Through knowledge transfer, a creative program was designed to improve patients’ rehabilitation experience. Among the implemented programs were:
1. Healthy Heart for Stroke: Designed to improve the endurance of stroke patients, this program was implemented as reduced endurance is a common complication of chronic stroke.
2. Gym for Active Elderly (GOAL): Aimed at encouraging the elderly to be active through physical activities conducted throughout the program, thus reducing their risk of stroke.
3. SCORE 0:2: With its ‘Zero In, Double Out’ policy, patients at SCORE might have minimal knowledge when they first enter the centre, but by the time they leave, they will gain at least twice the knowledge on health issues such as stroke. They will be educated on the risk factors, how to recognise stroke and the rehabilitation process.
4. StrokeCare Continuum: A long-term support and follow-up program designed to nurture stroke patients’ progress and empower them for a brighter future. With personalised care plans, telemedicine services and engaging peer support, StrokeCare continuum ensures continued success on the recovery journey.
Patient and Community benefits
Previously, there had been only 152 patients over a span of 8 years. However, since its inception in 2016, the number of patients has almost doubled, with an increase of over 100 patients. While the doubling of patients could have presented challenges, SCORE rose to the occasion by implementing an innovative model, which is a combination of improved resource allocation, communication enhancements, scalable infrastructure, an expanded medical team, data-driven insights, educational initiatives, and a commitment to continuous improvement. By transparently showcasing these measures, the centre can gain confidence in the stroke survivors’ ability to manage the increased patient load effectively and ensure a seamless experience for all involved. Additionally, SCORE addressed the previous issues of lack of trained manpower, old equipment, and failure to deliver effective programs to assist patients’ rehabilitation journeys. Today, the centre functions efficiently and, with its new infrastructure capabilities, no longer faces over-occupation, and more patients are benefiting from the project. This is indicative of the effectiveness of SCORE.
SCORE serves as a sustainable CBR that will continue to elevate the provision of care for the stroke community. With its ageing population, the occurrence of stroke in Malaysia will increase (Hwong et al. 2021); therefore, there is a need to promote stroke awareness, particularly primary prevention of stroke. The centre is close to Hospital Kuala Lumpur, an acute care centre, so our efforts have alleviated the congestion at the hospital by providing care at the community level. By providing further training for the physiotherapist at SCORE and implementing more programs, such as neurologic music therapy, we could potentially bring about a new age of treatment where CBR is the focal point of providing accessible and effective treatment to stroke patients. SCORE also provides a platform for previous patients to continue their rehabilitation in a community setting, which is more convenient for the patients and their careers. As a result, the patients are no longer reliant on receiving treatment from hospitals, reducing their healthcare expenditure. Through knowledge transfer to patients, the centre has become a beacon in the community as it provides stroke patients with improved and ongoing beneficial care through patient-centric education. As such, SCORE focuses on empowering patients so that, rather than perceiving themselves as passive recipients of charity, they are active and ongoing learners in their own care.
Overall, we have seen the following impacts:
1. Improved function of stroke survivors
2. Increased number of attendees at the centre
3. Improved quality of life
4. Shared and applied empirical knowledge in a real-world setting
5. Raised awareness of stroke
6. Improved access to rehabilitation facilities
7. Promoted wellbeing of elderly in the community.
Conclusion and next steps
Previously known as Pusat Pemulihan Kesihatan (PERKIM), SCORE transformed from a charity-based centre into a sustainable CBR centre that helps stroke survivors in underprivileged communities. The relationship created through this concept is in line with the principles introduced through the NBOS (Ministry of Human Resources, 2017). As a result, it increases community participation, while also involving experts who can provide professional input.
With its adherence to the recommended features of the World Health Organisation (WHO) CBR model, SCORE is an exemplary model for future stroke community rehabilitation centres in Malaysia. As 2030 approaches, there is a growing need to address WHO’s Rehabilitation 2030 initiative (World Health Organisation 2015). With the increasing number of people living with chronic diseases, providing access to rehabilitation is a growing concern (Yasin et al. 2012). Many individuals in underprivileged communities go without treatment due to the lack of resources (Abdul Aziz et al. 2014). Furthermore, Malaysia is a developing country, and 2.91 million households are in the lower income group, with a monthly income of less than RM 4,850 (Mahidin 2021). A majority of Malaysians are uninsured and cannot afford treatment at private hospitals. Hence, SCORE aims to provide them with the care that they need to avoid further complications and to uplift their quality of life.
Due to the success of SCORE, efforts are being made, in collaboration with PERKIM, to implement the resultant CBR model in other Malaysian states. Efforts are already being made to expand the reach of SCORE to the state of Kelantan by identifying the barriers to, and necessity of establishing a stroke rehabilitation centre in Kota Bharu. SCORE’s initiatives align with Sustainable Development Goal (SDG) 3.8, which aims to provide universal health coverage for all (United Nations 2015). These efforts also support SDG 4.7, which aims to provide learners with the right knowledge and skills needed to promote sustainable development (United Nations 2015). This could signal a new age of administering rehabilitation at the community level, in which SCORE could serve as the model for the future. This community-based rehabilitation model could radically change the landscape for stroke rehabilitation.
By extending research efforts to application within the community, many stroke survivors would benefit from the programs implemented. Hence, it is important to continue the research and further develop the project model to streamline implementation in other areas that require more CBRs.
In summary, the joint venture with PERKIM to extend the reach of SCORE aims to bridge the gap in provision of rehabilitation within the community by pivoting from a charity-based model to one that incorporates collaboration, sustainability, and multi-partnership with the university, industry, government and community. Through this, stroke survivors would be given agency over their own care, rather than being perceived as recipients of charity. Areas where access to medical rehabilitation is challenging would be emphasised because limited access to medical rehabilitation could lead to preventable declines in health and functional abilities. As a result, individuals in those communities would be faced with unsustainable healthcare costs in the long run due to the deteriorative nature of conditions that could have been effectively managed through timely rehabilitation. Hence, SCORE aims to target the communities that need these services the most.
References
Abdul Aziz, A, Mohd Nordin, N, Abd Aziz, N, Abdullah, S, Sulong, S & Aljunid, S 2014, ‘Care for post-stroke patients at Malaysian public health centres: Self-reported practices of family medicine specialists’, BMC Family Practice, vol. 15, no. 40. https://doi.org/10.1186/1471-2296-15-40
Akhavan Hejazi, S, Mazlan, M, Abdullah, S & Engkasan, J 2015, ‘Cost of post-stroke outpatient care in Malaysia’, Singapore Medical Journal, vol. 56, no. 2, pp. 116–19. https://doi.org/10.11622/smedj.2015025
Carayannis, E & Campbell D 2009, ‘“Mode 3’’ and “Quadruple helix”: Toward a 21st century fractal innovation ecosystem’, International Journal of Technology Management, vol. 46, nos. 3/4, pp. 201–34. https://doi.org/10.1504/IJTM.2009.023374
Clarke, D & Forster, A 2015, ‘Improving post-stroke recovery: The role of the multidisciplinary health care team’, Journal of Multidisciplinary Healthcare, vol. 8, pp. 433–42. https://doi.org/10.2147/JMDH.S68764
Department of Statistics Malaysia n.d., viewed 15 June 2022. http://www.dosm.gov.my
GBD 2015, Disease and Injury Incidence and Prevalence Collaborators 2016, Global, regional and national incidence, prevalence and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015, Lancet, vol. 388, no. 10053, pp. 1545–602. https://doi.org/10.1016/S0140-6736(16)31678-6
Hwong, W, Ang, S, Bots, M, Sivasampu, S, Selvarajah, S, Law, W, Latif, L & Vaartjes, I 2021, ‘Trends of stroke incidence and 28-day all-cause mortality after a stroke in Malaysia: A linkage of National Data Sources’, Global Heart, vol. 16, no. 1, p. 39. https://doi.org/10.5334/gh.791
Jee, R & Abdul Latif, L 2017, Return to work after stroke, 2nd JKWPKL & Putrajaya Research Day and 1st Hospital Rehabilitasi Cheras Research Day. https://doi.org/10.13140/RG.2.2.29992.62728
Mahidin, M 2021, Household income estimates and incidence of poverty report, Malaysia, 2020, viewed 15 June 2022. https://www.dosm.gov.my/portal-main/release-content/household-income-estimates-and-incidence-of-poverty-report-malaysia-2020
Ministry of Human Resources 2017, National Blue Ocean Strategy (NBOS), viewed 15 June 2022. https://mohr.gov.my/index.php/en/trade-union/9-site-content/75-nbos-archives?boxed=1
Mohd Zulkifly, M, Ghazali, S, Che Din, N & Subramaniam, P 2016, ‘The influence of demographic, clinical, psychological and functional determinants on post-stroke cognitive impairment at day care stroke center, Malaysia’, Malaysian Journal of Medical Sciences, vol. 23, no. 2, pp. 53–64. https://doi.org/10.1155/2016/3456943
Rutkowski, N, Sabri, E & Yang, C 2021, ‘Post-stroke fatigue: A factor associated with inability to return to work in patients <60 years-A 1-year follow-up’, PLOS One, vol. 16, no. 8, pp. e0255538. https://doi.org/10.1371/journal.pone.0255538
Tan, K & Venketasubramanian, N 2022, ‘Stroke burden in Malaysia’, Cerebrovascular Diseases Extra, vol. 12, no. 2, pp. 58–62. https://doi.org/10.1159/000524271
United Nations 2015, Transforming our world: The 2030 agenda for sustainable development, viewed 15 June 2022. https://sdgs.un.org/2030agenda
Yasin, S, Chan, C, Reidpath, D & Allotey, P 2012, ‘Contextualizing chronicity: A perspective from Malaysia’, Globalization and Health, vol. 8, p. 4. https://doi.org/10.1186/1744-8603-8-4